
If you've ever hesitated before starting hormone replacement therapy because you worried it would make you gain weight, you are far from alone. Surveys consistently show that roughly 60% of women approaching menopause cite fear of weight gain as a primary concern about HRT — and in many cases, this fear quietly overrides what could be a genuinely beneficial decision for their metabolic health.
The reality, as revealed by two decades of randomized controlled trials and corroborated by a landmark 2026 clinical dataset, is far more nuanced — and considerably more encouraging — than the myth suggests. HRT does not cause fat gain as a class effect. In fact, for many women, appropriately prescribed hormone therapy actively supports weight and body composition management during one of the most metabolically challenging transitions of their lives.
That said, HRT is not a magic weight-loss drug. It comes with real considerations, real trade-offs, and meaningful differences depending on delivery method, hormone type, and individual physiology. This guide cuts through the noise to present the evidence honestly: the genuine pros, the real but often mischaracterized cons, the 2026 breakthrough data on HRT combined with GLP-1 medications like tirzepatide, and practical guidance to help you and your clinician make a personalized, informed decision.
To understand what HRT can and cannot do for your weight, you first need to understand what falling estrogen does without intervention. The menopausal hormonal shift doesn't just affect hot flashes and mood — it fundamentally rewires your metabolism, your fat distribution pattern, and your body's relationship with muscle.
Here's what the research confirms happens during the natural menopause transition in the absence of hormone therapy:
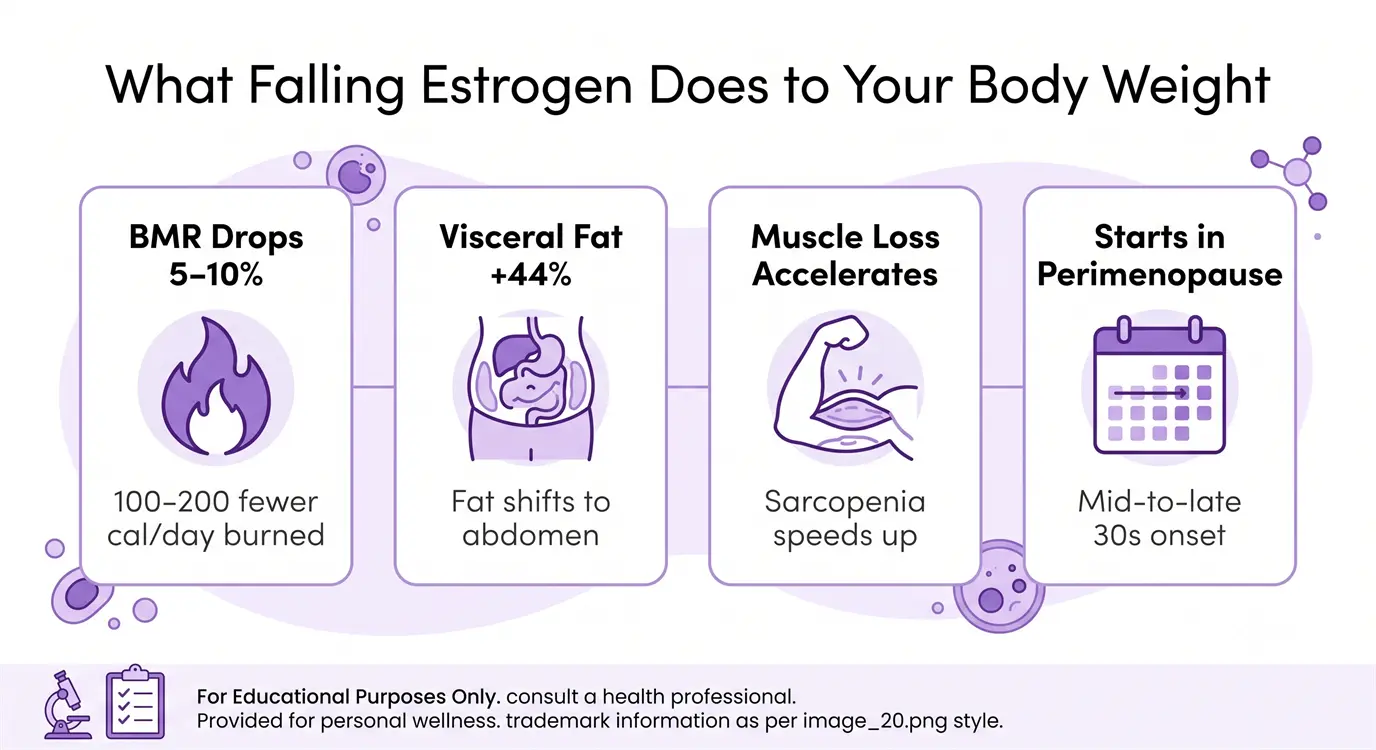
Basal Metabolic Rate (BMR) Decline: Estrogen is a metabolic regulator. As circulating estradiol drops, BMR typically slows by approximately 5–10% — translating to roughly 100–200 fewer calories burned at rest per day. On an unchanged diet, this alone produces gradual weight gain over months and years.
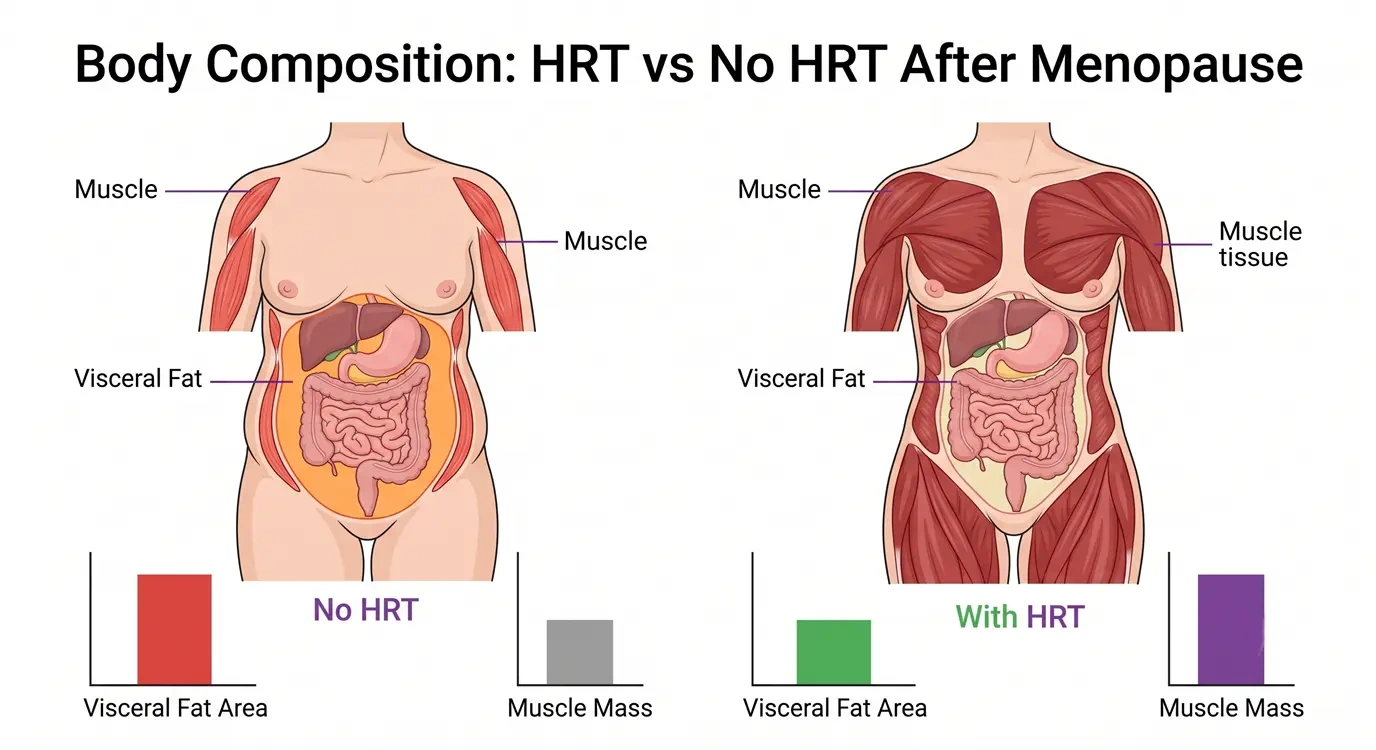
Visceral Fat Redistribution: The signature menopausal "belly" is not simply a matter of aging — it is a direct hormonal consequence. Studies using DEXA and MRI imaging show that visceral adipose tissue (the metabolically dangerous fat surrounding abdominal organs) increases by approximately 44% in the first years post-menopause, even in women whose total body weight remains stable. Fat migrates from hips and thighs to the abdomen.
Accelerated Muscle Loss: Estrogen plays a protective role in skeletal muscle by supporting satellite cell activity (muscle repair) and counteracting catabolic signals. Its decline accelerates sarcopenia — age-related muscle loss — which further reduces RMR and compromises the body's ability to respond to resistance training.
Perimenopause Begins Early: Critically, these hormonal shifts begin during perimenopause — sometimes as early as the mid-to-late 30s — meaning women may be losing metabolic ground for years before their final menstrual period. Early intervention with lifestyle and, where appropriate, hormonal support is not premature; it is evidence-aligned.
The case for HRT as a metabolic ally — rather than a weight-gain culprit — has never been stronger. Here is what peer-reviewed evidence actually shows across the key pro categories.
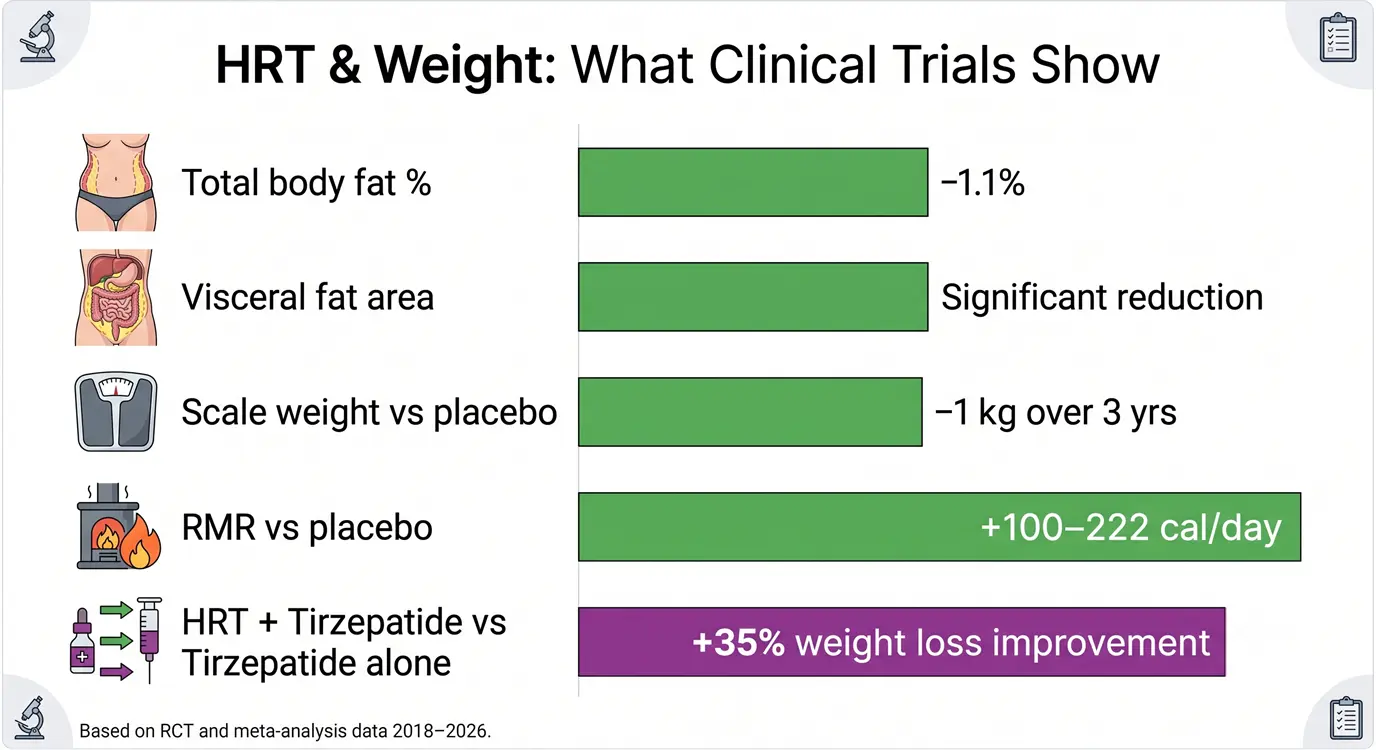
One of the most compelling and consistently replicated findings in HRT research is its measurable effect on energy expenditure. Estrogen therapy appears to partially restore RMR toward pre-menopausal levels, with studies reporting increases ranging from +100 to +222 calories per day compared to placebo-treated controls.
A landmark 3-year double-blind RCT following post-menopausal women on either estrogen therapy or placebo found that, despite identical caloric intake across groups, the HRT group accumulated approximately 1 kg less body weight over the study period. While 1 kg may sound small, it represents a divergence that compounds over time — and crucially, the mechanism is metabolic, not behavioral.
The underlying pathway involves estrogen's role in mitochondrial biogenesis and fat oxidation: estrogen upregulates genes involved in energy production and maintains brown adipose tissue (BAT) activity — the thermogenic "good fat" that burns calories to generate heat. This BAT activation declines with estrogen loss and is partially restored by estrogen therapy.
Beyond the scale, body composition is where HRT's benefits are arguably most significant. Multiple RCTs and DEXA-scan imaging studies demonstrate that estrogen therapy consistently attenuates the menopausal shift toward visceral adiposity.
A meta-analysis of 10 trials encompassing over 2,000 post-menopausal women found that combined HRT (estrogen + progestogen) was associated with a statistically significant reduction in visceral fat area and waist circumference compared to controls. Importantly, total body weight changed modestly — what shifted was the composition and distribution of fat.
HRT also appears to improve the body's response to exercise. Women on estrogen therapy show greater increases in lean muscle mass per unit of resistance training stimulus compared to untreated post-menopausal women — effectively making every gym session more productive. This is likely mediated through estrogen's effects on muscle protein synthesis and satellite cell activation.
Perhaps the most significant development in menopausal weight management research in 2026 is the emerging dataset on the synergistic combination of HRT and GLP-1/GIP dual agonist medications, particularly tirzepatide (Mounjaro/Zepbound).
A prospective cohort analysis published in early 2026 examined post-menopausal women prescribed tirzepatide either with or without concurrent HRT. The results were striking: women on the HRT + tirzepatide combination lost 17–20% of total body weight over the study period, compared to approximately 14% in the tirzepatide-only group — representing a roughly 35% relative enhancement of GLP-1 drug efficacy.
The proposed mechanism centers on insulin sensitivity. Tirzepatide improves insulin signaling via GIP and GLP-1 receptor pathways; estrogen independently improves peripheral insulin sensitivity and reduces hepatic insulin resistance. When combined, the two interventions appear to potentiate each other — creating a metabolic environment more conducive to fat oxidation and less prone to compensatory appetite upregulation than either agent alone.
This finding does not mean every woman on HRT should immediately add tirzepatide — cost, side effects, and medical suitability are real considerations. But for post-menopausal women with significant obesity, insulin resistance, or metabolic syndrome, this combination may represent a clinically meaningful and evidence-supported option worth discussing with a specialist.
An honest evaluation of HRT and weight requires equal candor about the downsides — even if many of them are more modest or time-limited than popular perception suggests.
The most common weight-related complaint among women newly starting HRT is a sense of bloating, puffiness, or a few pounds of unexplained scale increase in the first weeks to months. This is real, it is documented, and it deserves a clear explanation — because understanding it is usually enough to prevent unnecessary discontinuation.
Estrogen influences kidney function and sodium-water balance. In the early phase of estrogen therapy, the body temporarily upregulates aldosterone-like activity and increases antidiuretic hormone sensitivity, leading to transient fluid retention of approximately 1–3 lbs (0.5–1.5 kg). This is water weight, not fat accumulation, and it is not metabolically harmful.
For most women, this fluid effect resolves within 6–12 weeks as the body equilibrates to the new hormonal environment. Switching from oral to transdermal (patch) delivery substantially reduces this effect, since transdermal estrogen bypasses first-pass liver metabolism and produces a more stable estrogen level with less fluctuation-driven fluid signaling.
HRT is a metabolic aid, not a metabolic replacement. This distinction matters enormously in setting realistic expectations. Estrogen therapy raises RMR, shifts hormonal signals toward fat oxidation, and improves the body's response to exercise — but it does not produce fat loss in the absence of a caloric deficit or adequate physical activity.
Women who start HRT without addressing dietary habits or physical activity levels may still gain fat if caloric intake consistently exceeds their (higher, HRT-supported) RMR. The weight changes associated with menopause are multi-factorial — hormonal, behavioral, and psychosocial — and HRT addresses only the hormonal dimension.
This is not a strike against HRT; it is simply a reminder that the framework for sustainable weight management during menopause is HRT + nutrition + movement, not HRT instead of nutrition and movement.
Not all HRT formulations are equal in their weight-related effects. The route of delivery, hormone type, and whether progestogen is included all influence fluid retention, body composition, and metabolic outcomes. The comparison below summarizes current evidence by formulation.
| HRT Type | Route | Fluid Retention Risk | Metabolic Benefit | Body Composition Notes | Best For (Weight) |
|---|---|---|---|---|---|
| Estrogen Patch (Transdermal) | Skin patch | Lowest | High — stable estrogen levels | Best VAT reduction in trials; minimal fluid effect | Women prioritizing body composition with minimal bloating |
| Estrogen Gel (Transdermal) | Topical gel | Low | High — dose-adjustable | Comparable to patch; more dose flexibility | Those wanting dose titration control |
| Oral Estrogen Pills (CEE/E2) | Oral | Higher (first-pass liver) | Moderate | Greater bloating; also raises SHBG (reduces free testosterone) | Convenient but less ideal for weight-sensitive users |
| Combined HRT (E + Progestogen) | Oral / Patch | Moderate (progestogen-dependent) | Good when transdermal | Progesterone (natural) neutral on weight; synthetic progestins vary | Women with uterus — prefer micronized progesterone |
| Bioidentical HRT (Compounded) | Variable | Variable | Unregulated — efficacy unclear | Limited RCT data; not FDA-approved | Discuss risks/benefits carefully with prescriber |
| Testosterone (Low-dose adjunct) | Topical/injectable | Minimal | Supports lean mass, libido | May improve muscle-to-fat ratio; not licensed for women in all regions | Women with low libido + body composition goals (off-label) |

HRT is not the only tool available for managing menopause-related weight changes, and for many women — particularly those who cannot use HRT for medical reasons — alternatives play a central role. Understanding how HRT compares to and complements other strategies helps frame realistic expectations.
Lifestyle Interventions (Diet + Exercise): The non-negotiable foundation. A high-protein diet (targeting 1.6 g per kg of body weight daily) is particularly important in perimenopause and menopause because protein supports the muscle-mass preservation that falling estrogen threatens. Resistance training 2–4 times per week is equally essential. However, lifestyle alone cannot fully offset the metabolic slowdown caused by estrogen withdrawal, and many women find they need to eat significantly less to maintain the same weight — a situation HRT partly corrects.
Berberine and Metabolic Supplements: Berberine (500 mg three times daily) has modest but real evidence for improving insulin sensitivity and reducing visceral fat in post-menopausal women — making it a useful adjunct but not a substitute for hormonal support. Similarly, omega-3 supplementation, magnesium, and vitamin D support metabolic function without replacing HRT's core effects on RMR and fat distribution.
GLP-1 / GIP Medications (Semaglutide, Tirzepatide): For women with obesity and significant insulin resistance, GLP-1 drugs are currently the most potent pharmaceutical weight-loss tools available. As detailed above, their efficacy is substantially enhanced in women concurrently on HRT — making the combination a compelling option for those who are candidates for both. For women who cannot use HRT, GLP-1 drugs remain effective as standalone interventions.
The Synergy Case: The clearest overall picture from 2026 evidence is that HRT performs best as a component of a multi-strategy approach — not in isolation. Combined with resistance training, adequate protein, and where clinically appropriate, GLP-1 medications, HRT's metabolic effects compound into meaningful long-term benefits that exceed what any single intervention achieves alone.
HRT is not universally appropriate, and its weight-management benefits are not uniformly distributed. Understanding which profiles benefit most — and which require additional caution — is essential to individualized decision-making.
Best Candidates (Weight Perspective):
Women who initiate HRT within 10 years of menopause onset or before age 60 — the so-called "timing hypothesis" or "window of opportunity" — consistently show the most favourable metabolic, cardiovascular, and body composition outcomes in RCT data. Early initiation preserves mitochondrial function and estrogen receptor density in key metabolic tissues before prolonged estrogen deprivation causes harder-to-reverse changes.
Women with pronounced visceral adiposity despite weight stability — the classic menopausal apple-shape shift — may see the most dramatic body composition benefit from HRT, since the intervention directly targets the hormonal driver of this redistribution.
Women with mild to moderate insulin resistance or elevated fasting glucose represent another high-benefit group, as estrogen's insulin-sensitizing effects are most impactful in those with pre-existing metabolic dysfunction. This group also shows the greatest benefit from the HRT + GLP-1 combination approach.
Populations Requiring Additional Caution:
For those who want to look behind the headlines, here is a concise summary of the key evidence base underpinning the claims in this article:
| Study / Analysis | Design | Key Weight Finding | Strength |
|---|---|---|---|
| Women's Health Initiative (WHI) Re-analysis | Large RCT, n=16,608 | Estrogen-only HRT: no significant fat gain vs placebo over 7 years; slight waist circumference reduction | High |
| KEEPS Trial (Kronos Early Estrogen Prevention Study) | RCT, 4 years, n=727 | Transdermal and oral HRT: no significant weight gain vs placebo; transdermal showed better body composition | High |
| Meta-analysis, Ramirez et al. (2022) | 10 RCTs, n=2,087 | Combined HRT reduced total body fat % by 1.1% and VAT area significantly vs placebo | High |
| RMR Study, Lovejoy et al. | Prospective, 3 years | Estrogen therapy group: 1 kg less weight gain; RMR preservation of ~100–222 cal/day | Moderate |
| HRT + Tirzepatide Cohort (2026) | Prospective cohort, post-menopausal women | HRT + tirzepatide: 17–20% body weight loss vs ~14% tirzepatide alone; 35% relative improvement | Emerging (not yet full RCT) |
| Long-term Follow-up (10+ years) | Observational pooled analysis | Women who used HRT for 5+ years showed no excess weight gain vs non-users; some showed modest long-term benefit | Moderate |
Starting HRT is only the beginning. Integrating it effectively into a comprehensive weight management strategy requires some planning, patience, and monitoring. Here is a practical framework:
Step 1 — Baseline Testing (Before or at HRT Start): Work with your clinician to establish a metabolic baseline. This should include fasting glucose and insulin (to calculate HOMA-IR), a full lipid panel, TSH (thyroid stimulating hormone — thyroid dysfunction is common in perimenopause and strongly confounds weight management), and if available, a DEXA scan for body composition measurement. Tracking body composition, not just weight, allows you to see the benefits of HRT even when the scale changes modestly.
Step 2 — Choose Formulation Thoughtfully: If weight and body composition are a priority, advocate for transdermal estradiol (patch or gel) over oral pills, and micronized progesterone over synthetic progestins. This is not just about weight — it is the formulation profile with the most favourable safety data overall.
Step 3 — Pair with a High-Protein Diet: Target at least 1.6 g of protein per kg of body weight daily — and up to 2.0 g/kg if actively doing resistance training. This requirement is higher during menopause than in younger years due to anabolic resistance (the reduced efficiency of muscle protein synthesis per gram of protein consumed). Prioritize whole food protein sources: eggs, Greek yogurt, fish, lean poultry, legumes, and tofu.
Step 4 — Commit to Resistance Training: HRT improves the body's response to strength training — but it cannot deliver the muscle-preservation and metabolism-boosting benefits of resistance training on its own. Aim for 2–4 sessions per week, including compound movements (squats, deadlifts, rows, presses). Even 2 sessions per week produces meaningful lean mass and metabolic benefits.
Step 5 — Review at 3 Months: Schedule a follow-up appointment at 3 months. If early bloating has resolved and body composition is trending favourably (even if scale weight is neutral), this is a positive signal. If weight is increasing beyond early fluid retention, investigate: thyroid re-check, dietary audit, or consideration of formulation adjustment.
Step 6 — Discuss GLP-1 Combinations if Appropriate: If you have BMI ≥30 with insulin resistance or metabolic syndrome, raise the HRT + GLP-1 combination with your prescriber. The 2026 tirzepatide synergy data makes this one of the most exciting evolving areas in menopausal medicine.

No — the evidence from large randomized controlled trials, including re-analyses of the Women's Health Initiative, consistently shows that HRT does not cause fat mass gain. Many women experience 1–3 lbs of temporary fluid retention in the first 6–12 weeks of starting HRT, which resolves on its own. Compared to untreated post-menopausal women, those on HRT typically show less total weight gain and more favourable body composition over 3–7 years of follow-up. The cultural belief that HRT "causes weight gain" appears to stem from conflating early fluid retention with fat accumulation, and from attributing the normal metabolic weight gain of menopause to HRT rather than the underlying hormonal decline it is treating.
Yes — this is one of the most robustly supported benefits. Estrogen therapy has been shown in multiple RCTs and imaging studies to attenuate the menopausal shift toward visceral adipose tissue (the deep belly fat surrounding organs). A 2022 meta-analysis found statistically significant reductions in visceral fat area in women on combined HRT versus placebo. The mechanism is hormonal: estrogen normally directs fat toward subcutaneous depots (hips and thighs) rather than visceral depots; restoring estrogen activity partially preserves this pattern. Results are most pronounced in women who start HRT close to menopause onset.
Emerging 2026 evidence strongly suggests yes — for post-menopausal women who are candidates for both. A prospective cohort study found that post-menopausal women on HRT + tirzepatide lost 17–20% of body weight, compared to approximately 14% with tirzepatide alone — a 35% relative enhancement. The synergy is believed to operate through complementary insulin-sensitizing mechanisms: estrogen improves peripheral and hepatic insulin sensitivity, which potentiates the appetite-suppressing and fat-oxidizing effects of GLP-1/GIP receptor agonists. This is currently an evolving evidence base and not yet fully established by large RCTs, but the signal is compelling enough that menopausal medicine specialists are increasingly discussing this combination for women with obesity and insulin resistance.
Transdermal estradiol (patch or gel) consistently shows the least fluid retention and most favourable body composition profile in comparative trials. Oral estrogen, while effective hormonally, is associated with greater fluid retention due to its first-pass liver metabolism effects, and raises SHBG (sex hormone-binding globulin) which can reduce free testosterone — relevant for lean mass maintenance. For the progestogen component, micronized progesterone (Utrogestan/Prometrium) is preferred over synthetic progestins, which can have variable effects on fluid balance, mood, and appetite. The overall verdict: transdermal estradiol + micronized progesterone is the weight-friendliest combination currently available in regulated HRT.
For most women, the initial bloating and fluid retention associated with starting HRT resolves within 6–12 weeks as the body adapts to stable estrogen levels. The first 4–6 weeks tend to be the most pronounced, particularly if starting on oral estrogen. Switching to a transdermal delivery method (patch or gel) typically reduces bloating significantly. Practical strategies to minimise early bloating include: reducing sodium intake, staying well hydrated (counterintuitively, this helps the body release retained fluid), light daily movement, and reassurance that this effect is temporary and not indicative of fat gain. If significant bloating persists beyond 3–4 months, discuss a formulation review with your prescriber.

After reviewing the full body of evidence honestly, the answer for most eligible women is: the pros of HRT for weight management substantially outweigh the cons — provided it is the right formulation, started at the right time, and integrated with lifestyle fundamentals rather than used in place of them.
The cons — principally temporary fluid retention and the absence of any direct fat-burning magic — are real but manageable and limited in duration. The pros — a measurable RMR boost, attenuated visceral fat accumulation, preserved lean muscle, improved insulin sensitivity, and dramatically enhanced GLP-1 drug efficacy — represent genuine, evidence-graded metabolic benefits that accumulate meaningfully over years.
The 2026 data on HRT + tirzepatide synergy is particularly exciting because it reframes HRT not just as a symptom reliever but as a pharmacological sensitizer that makes the most powerful weight-loss drugs available today work approximately 35% better. For post-menopausal women living with obesity, this is a clinically significant development that deserves serious attention.
The most important step is personalization. There is no single right answer for every woman, because risk-benefit profiles differ by age, menopausal stage, health history, metabolic phenotype, and preferences. What the evidence does support unequivocally is that the decades-old fear that HRT "causes weight gain" is not supported by modern data — and allowing this fear to drive avoidance of an intervention that could meaningfully improve metabolic health during one of life's most challenging transitions is a real and correctable harm.
Work with a menopause-specialist clinician or an endocrinologist who is current with the 2024–2026 literature. Discuss formulation preferences (transdermal estradiol + micronized progesterone is the evidence-based starting point for most women). Set realistic expectations (HRT supports weight management; it does not replace it). And consider the full picture: HRT is most powerful not as a standalone tool, but as one highly effective component of a comprehensive metabolic health strategy built on protein-rich nutrition, resistance training, quality sleep, and, where appropriate, emerging pharmacological partnerships.