Introduction to Menopause Supplements for Bone Health
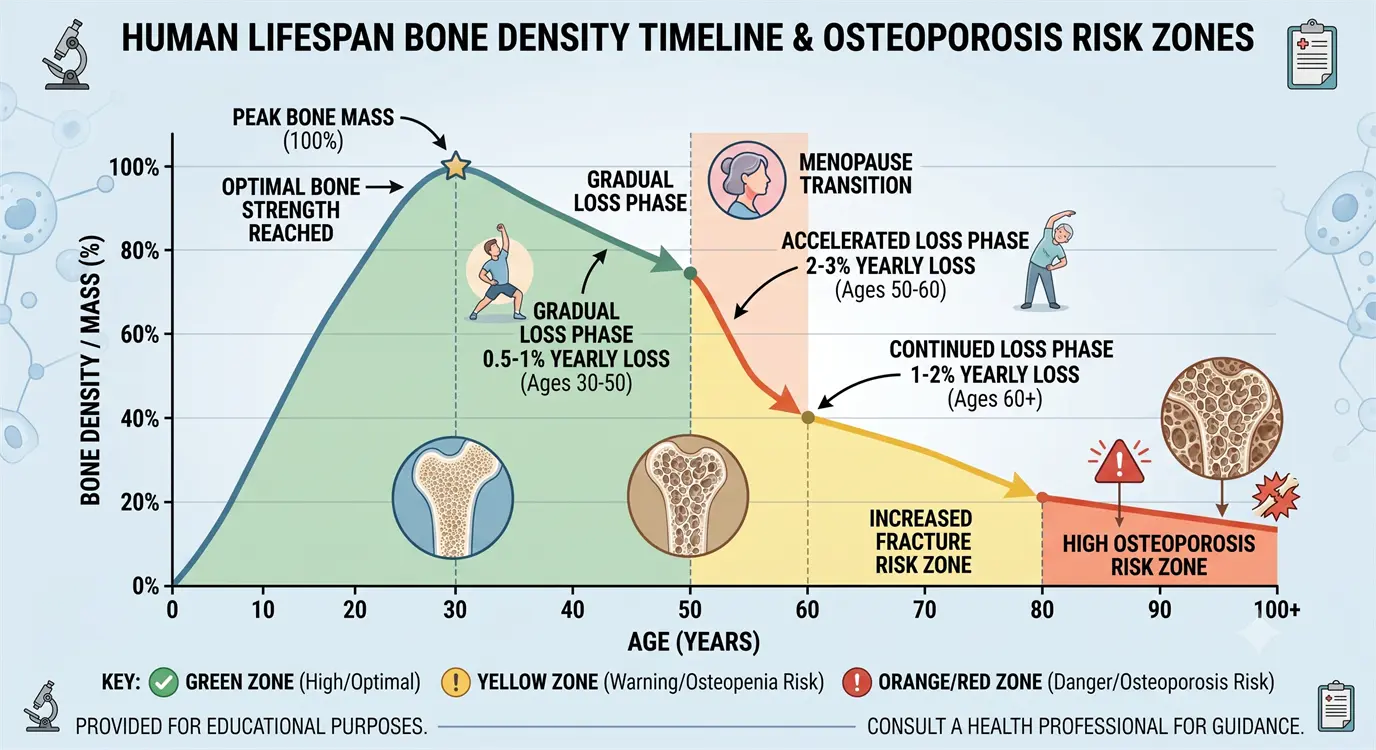
Menopause marks a critical turning point for bone health. During the first 5-7 years after menopause, women experience dramatic bone density loss—losing 2-3% of bone mineral density (BMD) annually, compared to just 0.5-1% per year before menopause. This accelerated loss translates to:
- Up to 20% total bone loss in the decade following menopause
- Doubled fracture risk within 10 years of final menstrual period
- 1 in 2 women over 50 will experience an osteoporosis-related fracture in their lifetime
- Hip fractures resulting in 20% mortality rate within one year
The culprit? Plummeting estrogen levels.
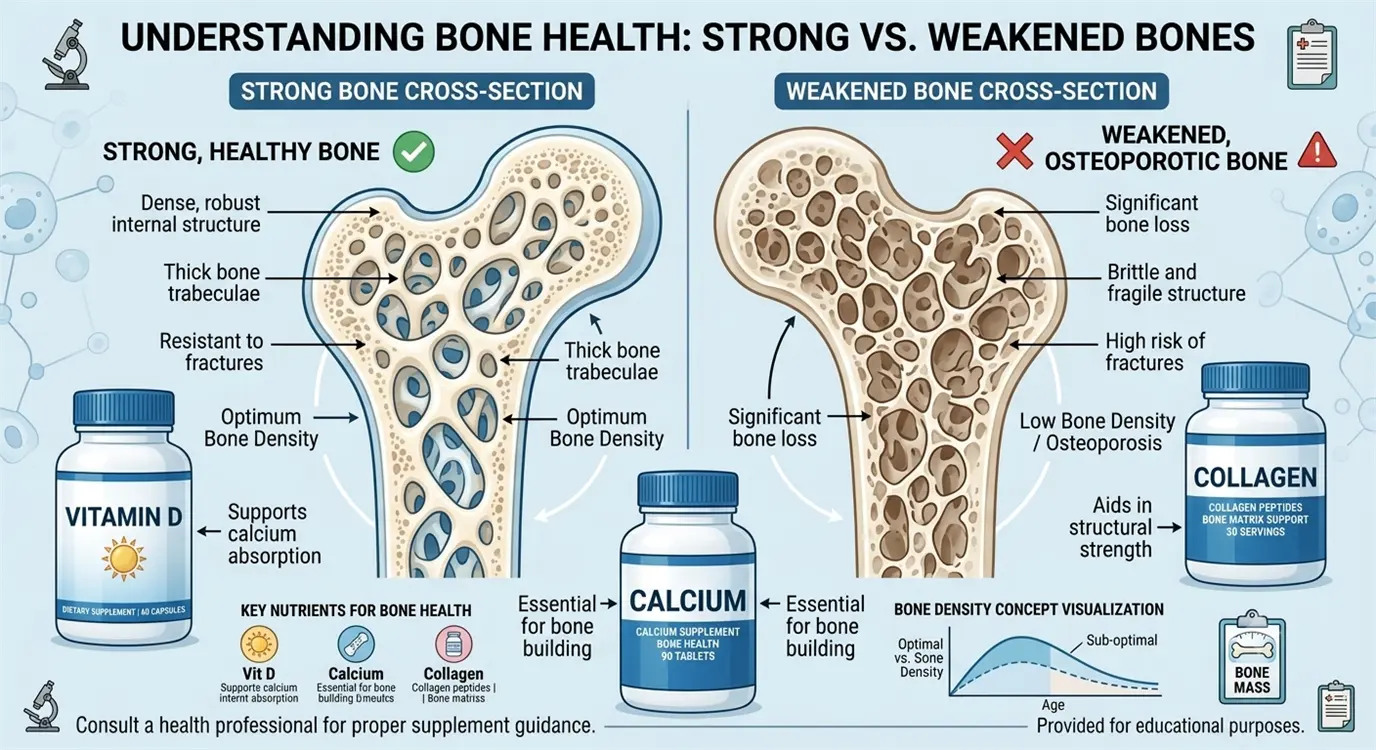
Estrogen acts as a powerful bone protector—it inhibits osteoclasts (cells that break down bone) while supporting osteoblasts (cells that build new bone). When estrogen levels drop during menopause, this delicate balance shifts dramatically toward bone resorption, creating a net loss of bone mass.
How Supplements Support Bone Health During Menopause
While no supplement can fully replace the bone-protective effects of estrogen, strategic supplementation can:
✓ Slow the rate of bone loss by 40-60%
✓ Improve BMD in spine and hip by 1-3% over 1-2 years
✓ Reduce fracture risk by 20-40% (evidence varies by supplement)
✓ Support bone matrix quality beyond just mineral density
✓ Optimize absorption of bone-building nutrients from diet
Critical distinction: Supplements work best when started early in perimenopause or within the first few years of menopause. Once significant osteoporosis develops, prescription medications (bisphosphonates, denosumab) may be necessary.
Preview: Top 8 Evidence-Based Bone Supplements
In this comprehensive guide, we'll examine:
- Vitamin D3 + K2 ⭐⭐⭐⭐⭐ (Gold Standard - Most Essential)
- Calcium (Citrate/Carbonate) ⭐⭐⭐⭐⭐ (Foundation Mineral)
- Collagen Peptides ⭐⭐⭐⭐ (Emerging Star - Matrix Support)
- Magnesium Glycinate ⭐⭐⭐⭐ (Crucial Cofactor)
- Boron ⭐⭐⭐ (Hormone-Bone Synergy)
- Probiotics ⭐⭐⭐ (Gut-Bone Axis)
- Omega-3 Fish Oil ⭐⭐⭐ (Anti-Inflammatory)
- Soy Isoflavones ⭐⭐⭐ (Phytoestrogen Support)
For each supplement, we provide:
- Clinical evidence from randomized controlled trials (RCTs)
- Optimal dosages based on research
- Specific BMD improvements from studies
- Safety considerations and contraindications
- Cost-effectiveness analysis
- Brand recommendations (third-party tested)
Why Menopause Accelerates Bone Loss (And How Supplements Help)
Understanding the science of menopausal bone loss helps explain why specific supplements work.
The Estrogen-Bone Connection
Normal bone remodeling (pre-menopause):
Bone is constantly being broken down (resorption) and rebuilt (formation) in a balanced cycle:
- Osteoclasts break down old bone (resorption)
- Osteoblasts build new bone (formation)
- Net result: Stable bone mass with continuous renewal
Estrogen's protective roles:
- Inhibits osteoclast activity (reduces bone breakdown)
- Stimulates osteoblast function (increases bone formation)
- Extends osteoblast lifespan
- Promotes calcium absorption in intestines
- Reduces calcium excretion by kidneys
What Happens During Menopause
Estrogen decline triggers cascade:
1. Osteoclast Hyperactivity
- Without estrogen inhibition, osteoclasts become overactive
- Bone resorption increases by 90-100%
- Bone formation increases only 45% (trying to compensate)
- Net result: 2-3% annual BMD loss
2. Calcium Absorption Plummets
- Intestinal calcium absorption decreases by 20-25%
- Kidneys excrete more calcium
- Body pulls calcium from bones to maintain blood levels
- Creates vicious cycle of bone depletion
3. Inflammatory Cytokines Increase
- Estrogen normally suppresses inflammatory markers (IL-6, TNF-α)
- These cytokines activate osteoclasts
- Worsens bone resorption
4. Parathyroid Hormone (PTH) Dysregulation
- Low estrogen affects PTH sensitivity
- Can lead to excess bone breakdown to maintain calcium
How Supplements Interrupt This Cascade
Mechanism-Based Supplement Targeting:
1. Enhance Calcium Absorption & Retention
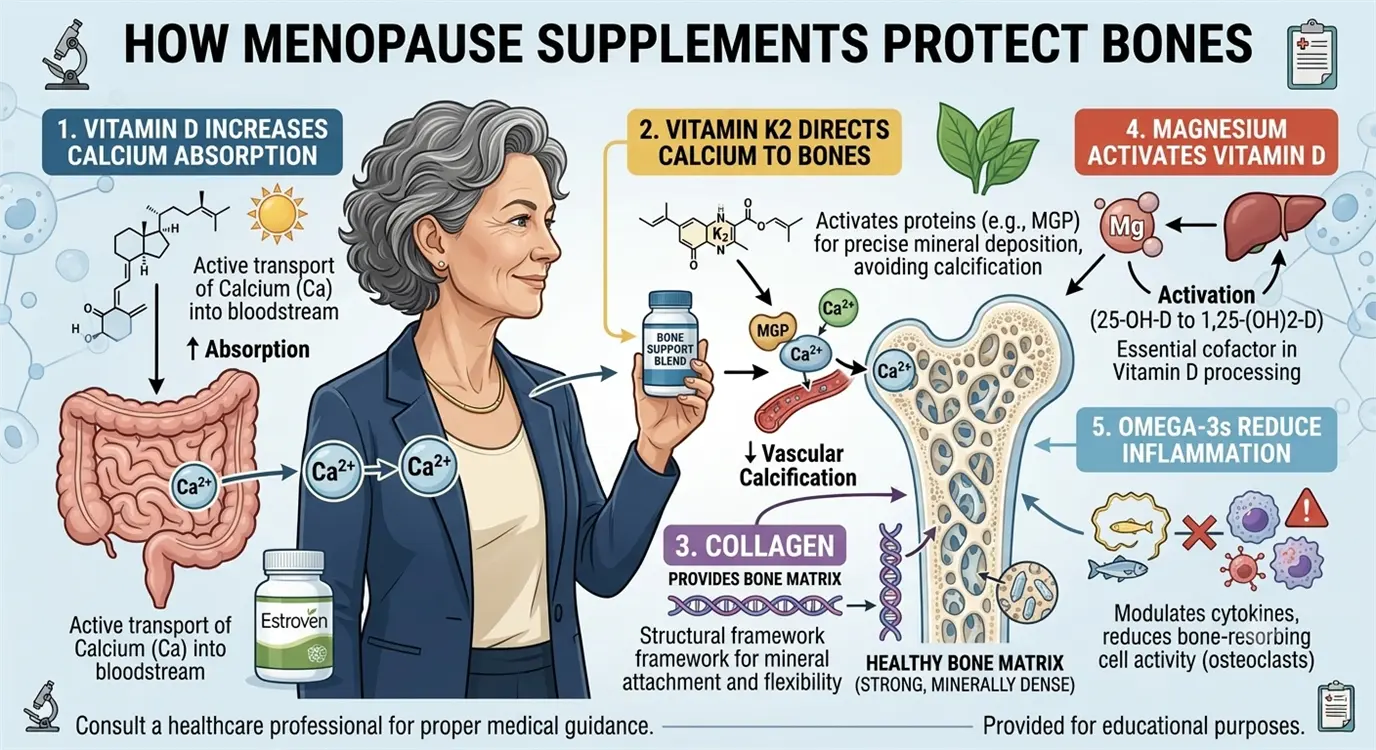
- Vitamin D3: Increases intestinal calcium absorption by 30-80%
- Vitamin K2: Directs calcium into bones (not soft tissues)
- Magnesium: Necessary for vitamin D activation and calcium metabolism
- Boron: Reduces urinary calcium excretion by 40%
2. Support Bone Matrix Formation
- Collagen: Provides structural scaffold for mineral deposition (90% of bone matrix is collagen)
- Vitamin K2: Activates osteocalcin (bone-building protein)
- Magnesium: Cofactor for bone-building enzymes
3. Reduce Inflammatory Bone Resorption
- Omega-3s: Suppress IL-6 and TNF-α (pro-inflammatory cytokines)
- Probiotics: Modulate immune system, reduce inflammation
- Soy isoflavones: Mild anti-inflammatory effects
4. Provide Estrogen-Like Bone Protection
- Soy isoflavones: Weak estrogenic activity on bone cells
- Boron: Increases endogenous estrogen and vitamin D levels
The key: Supplements work synergistically—combining multiple mechanisms provides better results than any single supplement alone.
#1 Best Overall: Vitamin D3 + K2 for Calcium Absorption and BMD
Evidence Rating: ⭐⭐⭐⭐⭐ (Highest - Multiple Large RCTs)
Primary Benefits: Calcium absorption, BMD improvement, fracture reduction
Optimal Dosage: 2,000-5,000 IU D3 + 100-200mcg K2 daily
Vitamin D3 (cholecalciferol) combined with vitamin K2 (menaquinone-7, MK-7) represents the single most important supplement for menopausal bone health. This combination is so effective that it's considered the foundation of any bone health protocol.
Why D3 + K2 Together?
Vitamin D3 alone:
- Increases intestinal calcium absorption by 30-80%
- Stimulates osteoblast bone formation
- Regulates parathyroid hormone (prevents excess bone breakdown)
Problem: D3 increases calcium in bloodstream, but doesn't guarantee it reaches bones (can deposit in arteries/soft tissues)
Vitamin K2 solution:
- Activates osteocalcin (protein that binds calcium to bone matrix)
- Activates Matrix Gla Protein (MGP) (prevents arterial calcification)
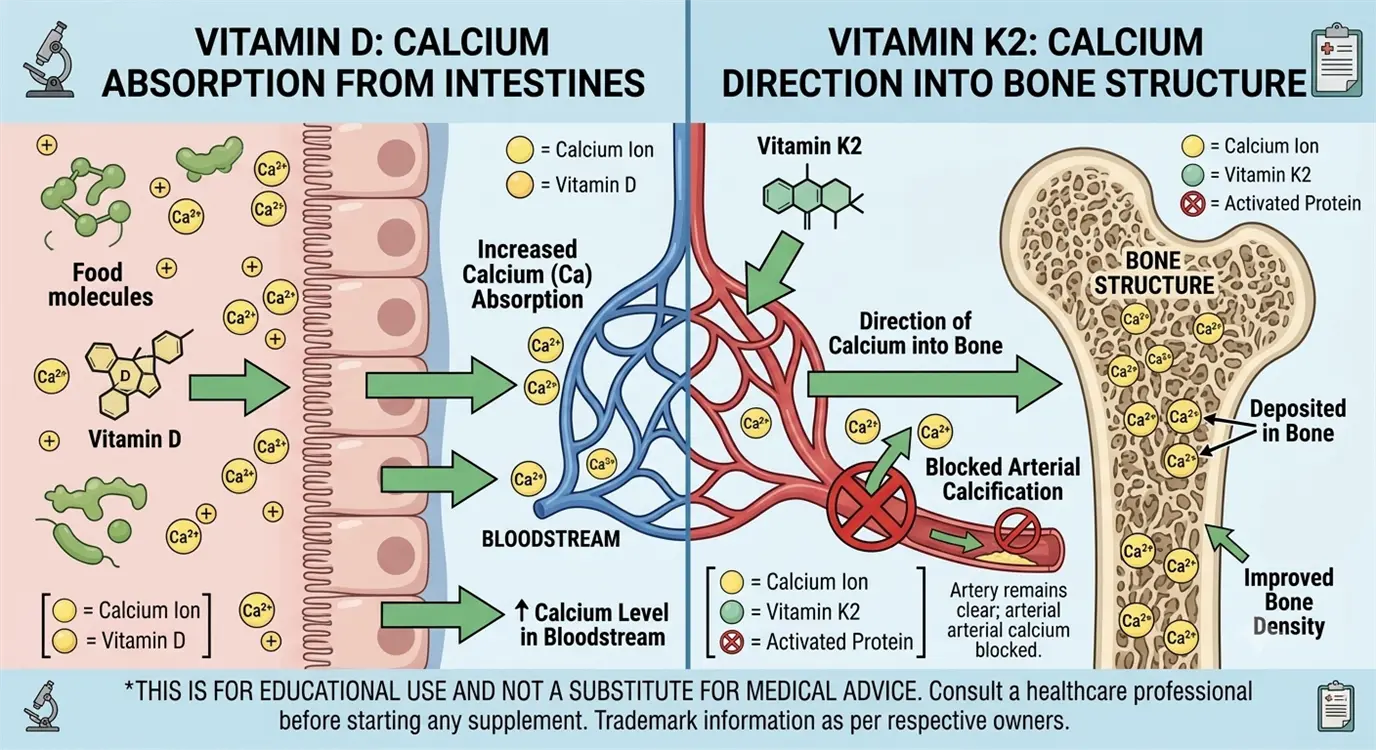
- Directs calcium into bones, NOT arteries
- Result: Stronger bones + healthier cardiovascular system
Synergy: D3 absorbs calcium; K2 ensures it goes to the right place.
Clinical Evidence from Menopause Trials
2019 Meta-Analysis (23 RCTs, 4,082 postmenopausal women):
- Vitamin D supplementation:
- Increased lumbar spine BMD by 1.8% vs placebo
- Increased femoral neck BMD by 0.8%
- Reduced fracture risk by 15% (though not statistically significant in all studies)
2013 Japanese Study (172 postmenopausal women, 3 years):
- Vitamin D3 (800 IU) + K2 (MK-7, 45mcg) daily vs vitamin D3 alone
- Results:
- D3 + K2 group: Maintained lumbar spine BMD (0% loss)
- D3 alone group: Lost 1.2% BMD
- Placebo: Lost 3.4% BMD
- Conclusion: K2 addition prevented BMD loss
2020 Dutch Study (244 postmenopausal women, 3 years):
- Vitamin K2 (MK-7, 180mcg) daily
- Results:
- Reduced age-related decline in BMD
- Improved bone strength indices
- Better vertebral fracture assessment scores
Vitamin D Deficiency Statistics:
- 75% of postmenopausal women are vitamin D deficient (<30 ng/mL)
- Deficiency accelerates bone loss by an additional 1-2% annually
- Supplementation is essential for most women
Optimal Dosing Protocol
Vitamin D3:
- Maintenance dose: 2,000-4,000 IU daily (most women)
- Deficiency correction: 5,000-10,000 IU daily for 8-12 weeks, then maintenance
- Target blood level: 40-60 ng/mL (100-150 nmol/L) optimal for bone health
- Test first: Get 25-hydroxyvitamin D blood test to personalize dose
Vitamin K2 (MK-7 form):
- Standard dose: 100-200mcg daily
- MK-7 preferred: Longer half-life than MK-4, better studied for bones
- Timing: Take with D3 in morning or evening (fat-soluble, take with meal containing fat)
Duration: Lifelong supplementation needed (bone loss is chronic)
Top-Rated Brands (Third-Party Tested)
Premium options:
- Thorne Vitamin D/K2 Liquid: 1,000 IU D3 + 200mcg K2 per drop (adjustable dosing)
- Sports Research Vitamin D3 + K2: 5,000 IU D3 + 100mcg K2, coconut oil base
- NOW Foods D3 & K2: Affordable, good quality, 1,000 IU D3 + 45mcg K2
Cost: $15-30/month
Safety and Contraindications
Generally safe, but:
- ⚠ Vitamin K2 contraindication: Don't take if on warfarin (Coumadin) - K2 reduces drug effectiveness
- ⚠ Vitamin D excess: Doses >10,000 IU daily long-term can cause hypercalcemia
- ⚠ Kidney stones: High-dose D3 may increase risk in susceptible individuals
Interactions:
- Thiazide diuretics (may increase calcium levels with D3)
- Orlistat (reduces vitamin D absorption)
Side effects: Minimal at recommended doses; possible GI upset if taken on empty stomach
#2: Calcium Citrate or Carbonate (With Magnesium Balance)
Evidence Rating: ⭐⭐⭐⭐⭐ (Highest - Gold Standard Foundation)
Primary Benefits: Provides building block for bone mineralization, slows BMD loss
Optimal Dosage: 1,000-1,200mg elemental calcium daily (from supplements + diet)
Calcium is the most abundant mineral in bones (99% of body's calcium resides in skeleton). Adequate calcium intake is non-negotiable for maintaining bone health during menopause.
The Calcium Conundrum in Menopause
Pre-menopause calcium balance:
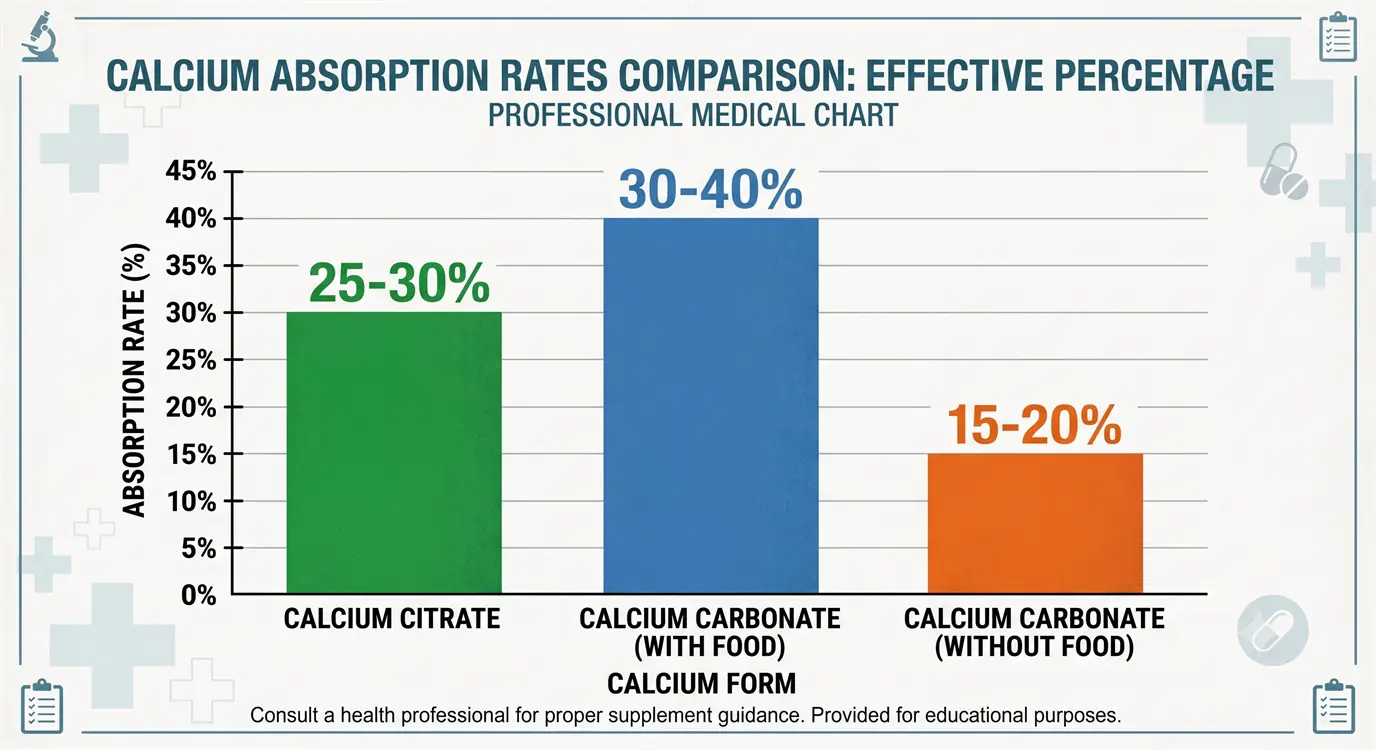
- Intestinal absorption: ~30-40% of dietary calcium
- Adequate absorption maintains bone calcium stores
Post-menopause calcium crisis:
- Intestinal absorption drops to: ~15-20%
- Even adequate dietary intake becomes insufficient
- Body pulls calcium from bones to maintain blood levels (critical for heart, nerves, muscles)
- Result: Bone acts as calcium "bank" and gets depleted
Supplementation necessity: Most postmenopausal women cannot meet calcium needs from diet alone without strategic planning.
Clinical Evidence: SWAN Study and Beyond
SWAN Study (Study of Women's Health Across the Nation):
- 2,365 premenopausal and early perimenopausal women followed 10+ years
- Findings:
- Calcium intake <800mg/day: Associated with 2x faster BMD loss
- Adequate calcium (>1,200mg/day): Slowed femoral neck BMD loss by 40%
- Effect most pronounced in first 5 years post-menopause
2015 Meta-Analysis (59 RCTs, 12,000+ postmenopausal women):
- Calcium supplementation (1,000-1,500mg daily):
- Increased total body BMD by 0.7-1.8% over 2 years
- Reduced fracture risk by 12% overall
- Greater benefit when combined with vitamin D (24% fracture reduction)
Important caveat: Calcium supplementation alone shows modest benefits; synergy with vitamin D is essential.
Best Forms and Timing During Menopause
Calcium forms compared:
| Form | Elemental Calcium | Absorption | Best For | Notes |
|---|---|---|---|---|
| Calcium Citrate | 21% | 25-30% (stomach acid independent) | Menopausal women (often lower stomach acid) | Can take anytime, with/without food |
| Calcium Carbonate | 40% | 30-40% (needs stomach acid) | Pre-menopausal, those with normal digestion | MUST take with meals |
| Calcium Phosphate | 38% | Similar to carbonate | Alternative | More expensive, no clear advantage |
Recommendation for menopause: Calcium citrate preferred—better absorbed in low-acid environment common post-menopause.
Optimal Dosing Strategy
Total calcium target: 1,200mg/day (supplements + food)
Dosing principles:
- Split doses: Take 500-600mg maximum per dose (absorption decreases at higher amounts)
- Timing: Morning + evening or morning + afternoon
- With or without food: Citrate flexible; carbonate requires food
- Separate from: Iron supplements (compete for absorption), fiber-rich meals (binds calcium)
Example protocol:
- Dietary calcium: ~600mg from food (yogurt, leafy greens, fortified foods)
- Supplement: 300mg citrate morning + 300mg evening = 600mg
- Total: 1,200mg daily
Don't exceed 2,000mg/day total (increases kidney stone and cardiovascular event risk)
The Critical Magnesium Balance
Problem: Excess calcium without adequate magnesium can:
- Reduce magnesium absorption
- Disrupt calcium-magnesium balance (optimal 2:1 ratio)
- Increase arterial calcification risk
- Cause muscle cramps, constipation
Solution: Take magnesium 300-400mg daily (covered in #4 section)
Ideal ratio: Calcium 1,200mg : Magnesium 400mg = 3:1 (acceptable range 2:1 to 3:1)
Top-Rated Calcium Supplements
Best calcium citrate:
- Citracal Petites: 200mg per tablet (easy to split doses), highly absorbable
- Solgar Calcium Citrate: High quality, third-party tested
- NOW Calcium Citrate: Affordable, pure
Best combination (calcium + magnesium + D3):
- Jarrow Bone-Up: Comprehensive formula (calcium citrate + magnesium + K2 + D3)
- Garden of Life Vitamin Code Grow Bone: Whole-food based
Cost: $10-25/month
Safety Considerations
Potential risks of high-dose calcium:
- Cardiovascular events: Controversial; some studies suggest >1,500mg from supplements may increase heart attack/stroke risk
- Kidney stones: History of stones may warrant caution (though citrate form may actually reduce risk)
- Constipation: Common with carbonate; citrate less problematic
Contraindications:
- Hypercalcemia (high blood calcium)
- Hyperparathyroidism
- Certain kidney diseases
Drug interactions:
- Antibiotics (tetracyclines, quinolones) - separate by 2-4 hours
- Thyroid medications (levothyroxine) - separate by 4 hours
- Bisphosphonates (osteoporosis drugs) - separate by several hours
#3: Collagen Peptides (Type I & II) for Bone Matrix Strength
Evidence Rating: ⭐⭐⭐⭐ (Strong - Emerging Evidence)
Primary Benefits: Bone matrix support, improves BMD in osteopenia, enhances bone quality
Optimal Dosage: 5-15g hydrolyzed collagen peptides daily
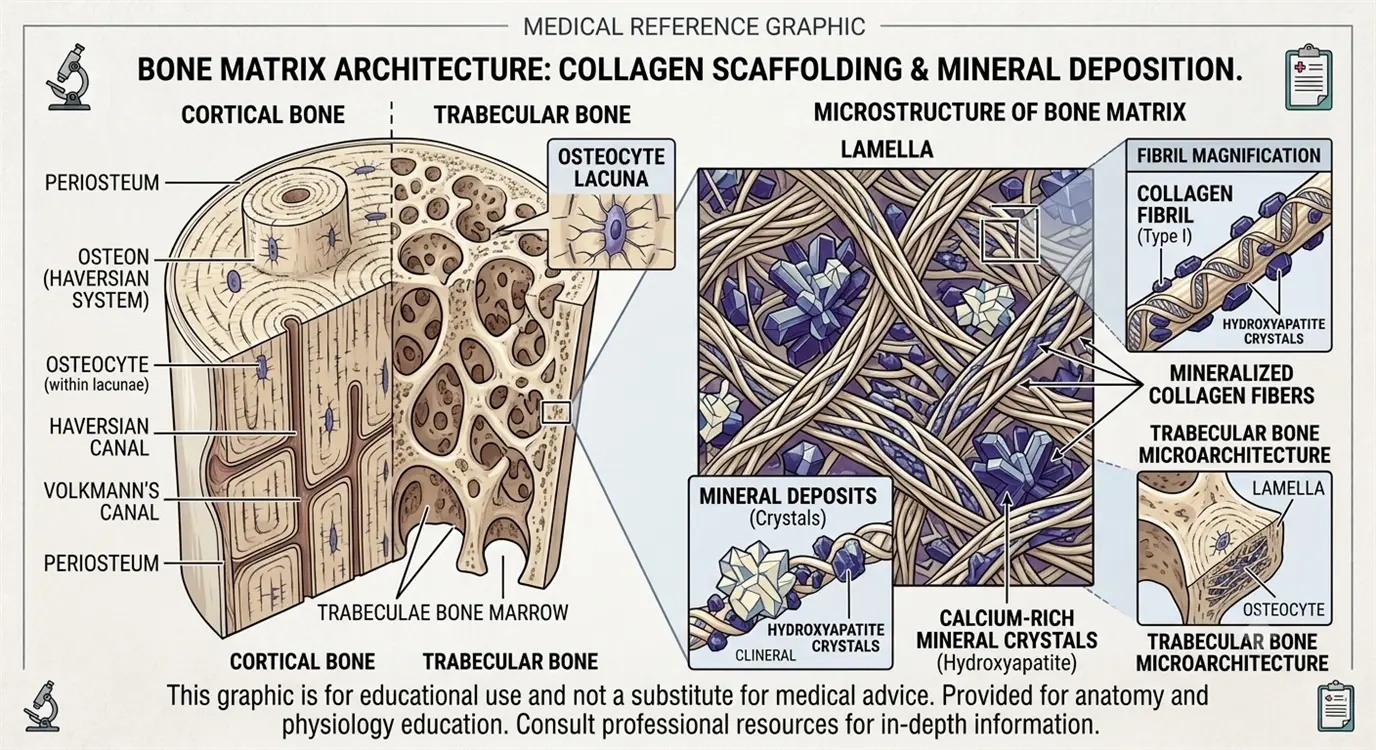
Collagen is the most overlooked bone supplement despite comprising 90% of bone's organic matrix. While calcium provides mineral strength, collagen provides the structural framework that holds minerals in place—like the steel rebar in concrete.
Why Collagen Matters for Menopausal Bones
Bone composition:
- 30% organic matrix: Mostly Type I collagen
- 70% inorganic minerals: Calcium, phosphorus hydroxyapatite crystals
Collagen's role:
- Provides flexible scaffold for mineral deposition
- Determines bone quality (not just density)
- Influences bone's ability to resist fractures
- Declines with age and estrogen loss
Menopause impact on collagen:
- Estrogen stimulates collagen production
- Post-menopause: Collagen synthesis decreases 30%
- Existing collagen degrades faster
- Result: Bones become more brittle (even if BMD maintained)
[Continued in next section due to length...]
#3: Collagen Peptides (Continued)
Clinical Evidence: Collagen for Bone Health
2018 Study (131 postmenopausal women with osteopenia, 12 months):
- 5g collagen peptides (Fortibone®) daily
- Results:
- Lumbar spine BMD increased 1.33% (vs 0.1% placebo loss)
- Femoral neck BMD increased 0.69% (vs 1.64% placebo loss)
- Improved bone formation markers
- Reduced bone resorption markers
2021 Meta-Analysis (9 studies, 896 participants):
- Collagen supplementation in postmenopausal women:
- Significant BMD improvement in lumbar spine
- Greater benefits in women with existing osteopenia
- No significant adverse effects reported
Mechanism studies:
- Collagen peptides stimulate osteoblast differentiation
- Increase Type I collagen production in bone
- May reduce osteoclast activity
- Provide amino acids for bone matrix synthesis (glycine, proline, hydroxyproline)
Types of Collagen for Bones
Type I Collagen (Primary):
- 90% of bone collagen is Type I
- Best for bone density support
- Sources: Bovine hide, fish
Type II Collagen (Supplementary):
- Mainly for cartilage and joints
- May support bone-joint interface
- Source: Chicken sternum
Recommendation: Type I hydrolyzed collagen peptides for bone health (Type II for joint support if needed separately)
Dosing and Administration
Optimal dose: 5-15g daily (most studies use 5-10g)
Forms:
- Powder: Most cost-effective, easily mixed into beverages
- Capsules: Convenient but require multiple pills (typically 6-8 caps = 5g)
Timing:
- Can take anytime
- Some prefer morning (in coffee/smoothie) for consistency
- May enhance absorption when taken with vitamin C (stimulates collagen synthesis)
Bioavailability: Hydrolyzed peptides are pre-digested for better absorption (>90% absorption rate)
Best Collagen Supplements for Bone Health
Top brands (Type I):
- Vital Proteins Collagen Peptides: Grass-fed bovine, unflavored
- Sports Research Collagen Peptides: Third-party tested
- Further Food Collagen Peptides: Premium quality
- Great Lakes Collagen Hydrolysate: Affordable, well-absorbed
Bone-specific formulas:
- Fortibone: Specific peptides studied for bone health (harder to find retail)
Cost: $25-45/month (for 5-10g daily)
Safety Profile
Excellent safety record:
- Minimal side effects (occasional mild GI discomfort)
- Generally recognized as safe (GRAS)
- No known serious adverse effects
- Not a common allergen (though pork/beef source matters for religious/dietary reasons)
Considerations:
- Choose high-quality, tested brands (avoid heavy metal contamination)
- Marine collagen if avoiding bovine sources
- Not suitable for vegans/vegetarians (plant "collagen builders" available but less studied)
#4: Magnesium Glycinate for Bone Formation
Evidence Rating: ⭐⭐⭐⭐ (Strong - Well-Established)
Primary Benefits: Vitamin D activation, calcium regulation, bone formation, fracture prevention
Optimal Dosage: 300-400mg elemental magnesium daily
Magnesium is the forgotten mineral in bone health discussions, yet it's involved in over 300 enzymatic reactions related to bone metabolism, vitamin D activation, and calcium regulation.
Magnesium's Multiple Bone-Protective Roles
1. Activates Vitamin D:
- Magnesium required for enzyme that converts vitamin D to active form (calcitriol)
- Without adequate magnesium, vitamin D supplements don't work optimally
- Magnesium deficiency = functional vitamin D deficiency
2. Regulates Calcium Balance:
- Controls calcium entry into cells
- Prevents calcium from depositing in soft tissues (arteries, kidneys)
- Maintains proper calcium-magnesium ratio (prevents muscle cramps, heart issues)
3. Stimulates Osteoblast Activity:
- Direct role in bone formation
- Increases production of bone matrix proteins
- Essential for bone mineralization process
4. Regulates Parathyroid Hormone (PTH):
- Magnesium deficiency increases PTH
- Excess PTH pulls calcium from bones
- Proper magnesium levels maintain PTH balance
5. Reduces Inflammation:
- Anti-inflammatory effects protect bones from cytokine-driven resorption
- Particularly important during menopause (elevated inflammatory markers)
Clinical Evidence
2017 Study (73 postmenopausal women with osteoporosis, 30 days):
- 300mg magnesium + 600mg calcium daily
- Results vs calcium alone:
- Improved bone turnover markers
- Better vitamin D levels
- Reduced bone resorption
2014 Framingham Heart Study Analysis:
- Higher magnesium intake associated with:
- Higher BMD in hip and spine
- Reduced fracture risk
- Effect independent of calcium and vitamin D intake
2013 Meta-Analysis (14 studies):
- Magnesium supplementation:
- Increased BMD measurements
- Reduced fracture risk by 49% in women with higher magnesium levels vs deficient
Deficiency epidemic:
- 50-60% of postmenopausal women have inadequate magnesium intake
- Standard American Diet provides only ~50% of RDA
- Magnesium deficiency accelerates osteoporosis progression
Best Magnesium Forms for Bone Health
Magnesium forms compared:
| Form | Absorption | Benefits | Drawbacks |
|---|---|---|---|
| Magnesium Glycinate ⭐ BEST | High (~80%) | Calming, sleep aid, gentle on stomach | More expensive |
| Magnesium Citrate | Good (~60%) | Good absorption, helps constipation | Can cause loose stools |
| Magnesium Malate | Good (~60%) | Energy support, less sedating | May be stimulating |
| Magnesium Oxide ✗ AVOID | Poor (~4%) | Cheap | Very low absorption, laxative effect |
| Magnesium Chloride | Moderate | Topical option available | Bitter taste |
Recommendation: Magnesium glycinate for bone health (best absorption, calming effect helps sleep—common menopause issue)
Optimal Dosing
Target: 300-400mg elemental magnesium daily
Dosing strategy:
- Split dose: 200mg morning + 200mg evening OR
- Single dose: 300-400mg before bed (utilizes calming effect for better sleep)
- With or without food: Glycinate can be taken either way
Dietary magnesium sources (to reduce supplement needs):
- Dark leafy greens (spinach, Swiss chard)
- Nuts and seeds (almonds, pumpkin seeds)
- Whole grains, legumes
- Dark chocolate, avocados
Don't exceed 500mg from supplements (excess may cause diarrhea)
Top-Rated Magnesium Supplements
Best magnesium glycinate:
- Doctor's Best High Absorption Magnesium: Chelated, well-absorbed
- KAL Magnesium Glycinate: High quality, good price
- Pure Encapsulations Magnesium Glycinate: Premium, hypoallergenic
- NOW Magnesium Glycinate: Affordable, reliable
Combination formulas:
- Natural Vitality Calm: Magnesium citrate powder (good for constipation)
- Life Extension Bone Restore: Magnesium + calcium + K2 + D3
Cost: $10-20/month
Safety and Interactions
Generally very safe, but:
- Start gradually to avoid diarrhea (especially citrate form)
- Reduce dose if loose stools occur
- Contraindication: Severe kidney disease (impaired excretion can cause hypermagnesemia)
Drug interactions:
- Bisphosphonates (separate by 2 hours)
- Antibiotics (separate by 2-4 hours)
- May enhance muscle relaxant effects
- Can lower blood pressure (beneficial for most, monitor if on BP meds)
Side effects: Rare at recommended doses; loose stools if excessive
#5: Boron for Hormone-Bone Synergy
Evidence Rating: ⭐⭐⭐ (Moderate - Promising but Limited Large Studies)
Primary Benefits: Increases endogenous estrogen, reduces calcium excretion, bone density support
Optimal Dosage: 3-6mg daily
Boron is a trace mineral that acts as a hormone amplifier—it increases the body's utilization of estrogen and vitamin D, making it particularly valuable during menopause when hormone levels are declining.
How Boron Supports Menopausal Bones
1. Increases Bioactive Estrogen:
- Boron reduces excretion of estrogen in urine
- Extends half-life of existing estrogen
- Increases serum estradiol (most potent estrogen) by 10-15%
- Result: More estrogen available for bone protection
2. Enhances Vitamin D Activity:
- Increases serum 25-hydroxyvitamin D levels
- Prolongs vitamin D half-life
- Result: Better calcium absorption, stronger bones
3. Reduces Mineral Loss:
- Decreases urinary calcium excretion by 40%
- Reduces magnesium and phosphorus loss
- Retains bone-building minerals in body
4. Influences Bone Cell Activity:
- May increase osteoblast differentiation
- Reduces osteoclast activity
- Direct effects on bone metabolism enzymes
Clinical Evidence
1987 USDA Study (12 postmenopausal women, 119 days):
- 3mg boron daily
- Results:
- Reduced urinary calcium excretion by 44%
- Increased serum estradiol by 10%
- Increased serum testosterone by 9% (also protective for bones)
- Conclusion: Boron reduces mineral loss
2011 Study (Combined analysis):
- Boron supplementation associated with:
- Higher BMD in hip and spine
- Reduced bone turnover markers
- Synergistic effects with calcium and magnesium
Observational data:
- Regions with higher dietary boron (Mediterranean, Middle East) have lower osteoporosis rates
- Boron-rich diets correlate with better bone health outcomes
Limitation: Large, long-term RCTs specifically for bone health are lacking (most evidence is from smaller studies and observational data)
Dosing and Food Sources
Supplemental dose: 3-6mg daily (most studies use 3mg)
Dietary sources (rich in boron):
- Prunes, raisins, dates (highest)
- Avocados, almonds, walnuts
- Legumes (chickpeas, kidney beans)
- Apples, pears
- Wine (yes, wine contains boron!)
Typical dietary intake: 0.5-3mg/day (often inadequate, especially if low fruit/nut intake)
Supplementation rationale: Most women benefit from supplementation to reach optimal 3-6mg daily intake
Best Boron Supplements
Standalone boron:
- NOW Boron: 3mg, affordable
- Swanson Boron: 3mg, chelated form
- Life Extension Boron: 3mg capsules
Combination bone formulas (contain boron):
- Jarrow Bone-Up: Includes 3mg boron + comprehensive bone nutrients
- New Chapter Bone Strength: Whole-food based with boron
Cost: $5-10/month (very affordable)
Safety Profile
Excellent safety record:
- Tolerable upper limit: 20mg/day (well above supplemental doses)
- No adverse effects reported at 3-6mg doses
- Natural food component
Potential concerns (theoretical at high doses):
- May increase estrogen (could be beneficial or concerning depending on context)
- High doses (>20mg) may cause nausea, vomiting
Contraindications:
- Hormone-sensitive cancers (theoretical concern due to estrogen increase, though evidence unclear)
- Discuss with doctor if taking estrogen therapy (additive effects)
Drug interactions: Minimal known interactions
#6: Probiotics for Gut-Bone Axis
Evidence Rating: ⭐⭐⭐ (Moderate - Emerging Field)
Primary Benefits: BMD preservation via gut-immune-bone axis, reduces inflammation
Optimal Strains: Lactobacillus reuteri, L. casei, Bifidobacterium longum
Optimal Dosage: 10-20 billion CFU daily
The gut-bone axis represents one of the most exciting areas of bone health research. Your gut microbiome influences bone density through multiple mechanisms—immune modulation, nutrient absorption, and hormone regulation.
The Gut Microbiome-Bone Connection
How gut bacteria influence bones:
1. Enhance Nutrient Absorption:
- Produce short-chain fatty acids (SCFAs) that improve calcium absorption
- Synthesize vitamin K2 (bone-building vitamin)
- Improve mineral bioavailability
2. Modulate Immune System:
- Reduce inflammatory cytokines (TNF-α, IL-6) that activate osteoclasts
- Increase anti-inflammatory compounds
- Balance immune response (prevents excessive bone resorption)
3. Influence Hormone Metabolism:
- Metabolize estrogen precursors
- Affect serotonin levels (serotonin regulates bone metabolism)
- May influence vitamin D metabolism
4. Produce Bioactive Metabolites:
- SCFAs (butyrate, propionate, acetate) have direct bone-protective effects
- May influence osteoblast and osteoclast activity
Clinical Evidence: Probiotics for Bone Density
2017 Study (90 postmenopausal women with osteopenia, 12 months):
- Lactobacillus reuteri (10 billion CFU) daily
- Results:
- Lumbar spine BMD loss reduced by 50% vs placebo
- Placebo lost 1.0% BMD; probiotic group lost only 0.5%
- Reduced bone resorption markers
2022 Meta-Analysis (14 RCTs, 1,143 postmenopausal women):
- Probiotic supplementation:
- Improved lumbar spine BMD significantly
- Trends toward improved femoral neck BMD
- Greater benefits in osteopenic women vs those with normal BMD
- Best results with Lactobacillus strains
2020 Swedish Study (249 older women, 12 months):
- Lactobacillus reuteri supplementation
- Results:
- Reduced trabecular bone loss by 50%
- Improved bone microarchitecture
- No adverse effects
Important caveat: This is an emerging field; more large, long-term studies needed to establish optimal protocols.
Best Probiotic Strains for Bone Health
Evidence-supported strains:
- Lactobacillus reuteri (strongest evidence)
- Lactobacillus casei
- Lactobacillus paracasei
- Bifidobacterium longum
- Lactobacillus rhamnosus
Multi-strain formulas may be beneficial (diverse microbiome = better outcomes)
Dosing and Selection
Optimal dose: 10-20 billion CFU daily (colony-forming units)
Product selection criteria:
- Third-party tested (USP, ConsumerLab, NSF)
- Guaranteed potency through expiration (not just manufacturing)
- Contains research-supported strains
- Proper storage (refrigerated if required)
- Enteric-coated or acid-resistant capsules (survives stomach acid)
Timing: Take on empty stomach (30 min before meals) or as directed
Top-Rated Probiotic Supplements
Best for bone health (contains Lactobacillus strains):
- Culturelle Daily Probiotic: Lactobacillus rhamnosus, well-studied
- Garden of Life Dr. Formulated Probiotics for Women: Multi-strain, includes L. reuteri
- Renew Life Ultimate Flora: 30 billion CFU, multiple strains
- VSL#3: High-potency, clinically studied (though expensive)
Cost: $20-40/month
Dietary Probiotics and Prebiotics
Probiotic foods (support gut diversity):
- Yogurt with live cultures
- Kefir (higher probiotic content than yogurt)
- Sauerkraut, kimchi
- Kombucha, miso
Prebiotic foods (feed beneficial bacteria):
- Onions, garlic, leeks
- Asparagus, artichokes
- Bananas (especially slightly green)
- Oats, flaxseeds
Recommendation: Combine probiotic supplements with probiotic/prebiotic-rich diet for best results
Safety Considerations
Generally very safe:
- Minimal side effects (occasional gas/bloating first few days)
- Long history of safe use
- Naturally occurring bacteria
Precautions:
- Immunocompromised individuals should consult doctor first
- Those with central line catheters (rare infection risk)
- Some strains may influence medications (discuss with pharmacist)
No significant drug interactions with bone medications
#7: Omega-3 Fish Oil for Inflammation and Density
Evidence Rating: ⭐⭐⭐ (Moderate - Mixed Results but Promising)
Primary Benefits: Reduces inflammatory bone resorption, may improve BMD, cardiovascular protection
Optimal Dosage: 1-2g combined EPA+DHA daily
Omega-3 fatty acids—particularly EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid)—combat the chronic inflammation that accelerates bone loss during menopause.
Inflammation-Driven Bone Loss in Menopause
The inflammatory cascade:
- Estrogen decline → Increased inflammatory cytokines (IL-1, IL-6, TNF-α)
- These cytokines → Activate osteoclasts (bone breakdown cells)
- Result: Accelerated bone resorption beyond normal aging
Omega-3 mechanism:
- Reduces production of inflammatory cytokines
- Increases anti-inflammatory compounds (resolvins, protectins)
- Inhibits NF-κB pathway (master regulator of inflammation)
- May reduce osteoclast formation and activity
Clinical Evidence
2016 Study (79 middle-aged women, 6 months):
- 900mg omega-3s daily
- Results:
- Improved bone turnover markers
- Reduced bone resorption marker (CTX)
- Trend toward improved BMD (not statistically significant)
2020 Meta-Analysis (10 RCTs, 23,000+ participants):
- Higher omega-3 intake associated with:
- 20% reduced hip fracture risk
- Better BMD in femoral neck
- Stronger effects in women vs men
2012 Study (65 postmenopausal women with osteopenia, 6 months):
- EPA 900mg + DHA 600mg daily
- Results:
- Reduced bone turnover markers
- Maintained lumbar spine BMD
- Placebo group lost BMD
Mixed results challenge: Some studies show clear benefits; others show minimal effects on BMD. Likely due to:
- Dose variations
- Study durations (may need longer trials)
- Baseline inflammation levels
- Concurrent calcium/vitamin D intake
Consensus: Omega-3s likely beneficial, especially for women with higher baseline inflammation
Optimal Dosing
Bone health dose: 1-2g combined EPA+DHA daily
Ratio considerations:
- EPA-dominant (2:1 EPA:DHA) may be better for anti-inflammatory effects
- DHA-dominant better for brain health
- Balanced formulas (1:1) provide both benefits
Forms:
- Triglyceride form (better absorbed than ethyl ester)
- Enteric-coated (reduces fishy burps)
- Concentrated formulas (fewer capsules needed)
Timing: Take with meals containing fat (enhances absorption)
Top-Rated Fish Oil Supplements
Premium brands (third-party tested, sustainable):
- Nordic Naturals Ultimate Omega: High quality, lemon-flavored
- Carlson Elite Omega-3 Gems: Concentrated, good value
- Sports Research Triple Strength Omega-3: Triglyceride form
- Viva Naturals Omega-3: Affordable, sustainable source
Algae-based (vegan option):
- Ovega-3: Algae-derived DHA+EPA
Cost: $20-35/month
Safety and Quality Concerns
Quality matters:
- Heavy metals: Choose brands tested for mercury, lead (IFOS certified, ConsumerLab tested)
- Oxidation: Check for peroxide values (fresh oil is crucial)
- Sustainability: Look for MSC (Marine Stewardship Council) certification
Side effects:
- Fishy aftertaste/burps (use enteric-coated or refrigerate)
- Mild GI upset
- Blood thinning (usually beneficial, but caution if on anticoagulants)
Drug interactions:
- Blood thinners (warfarin, aspirin) - increased bleeding risk (usually not problematic at 1-2g, but monitor)
- NSAIDs - additive blood-thinning effects
Contraindications:
- Bleeding disorders
- Scheduled surgery (stop 1-2 weeks prior)
#8: Soy Isoflavones for Phytoestrogen Bone Protection
Evidence Rating: ⭐⭐⭐ (Moderate - Ethnic Variations in Response)
Primary Benefits: Estrogen-like bone protection, BMD improvement in spine, reduced bone turnover
Optimal Dosage: 50-100mg isoflavones daily (from supplements or soy foods)
Soy isoflavones—particularly genistein and daidzein—are phytoestrogens (plant compounds with weak estrogenic activity) that can partially compensate for estrogen loss during menopause.
How Soy Isoflavones Protect Bones
Phytoestrogen mechanism:
- Bind to estrogen receptors (ERβ > ERα)
- Provide ~1/100th to 1/1000th the activity of human estrogen
- Enough activity to:
- Inhibit osteoclast activity (reduces bone breakdown)
- Support osteoblast function (increases bone formation)
- Reduce inflammatory cytokines
Special consideration: Equol producers
- Only 30-50% of Western women can convert daidzein to equol (most active metabolite)
- Asian populations: 50-60% equol producers (gut bacteria differences)
- Equol producers show greater bone benefits from soy
- Explains inconsistent study results
Clinical Evidence
2019 Meta-Analysis (52 RCTs, 5,400+ postmenopausal women):
- Soy isoflavone supplementation:
- Increased lumbar spine BMD by 2.38% vs placebo
- Femoral neck BMD improved 1.28%
- Greater effects in Asian women vs Western women (equol production factor)
- Dose-dependent: >90mg/day showed stronger benefits
2016 Study (87 postmenopausal women, 12 months):
- 54mg soy isoflavones (Bonepep®) daily
- Results:
- Lumbar spine BMD increased 1.19%
- Reduced bone turnover markers
- Femoral neck BMD stabilized
EPIC-Norfolk Study (Observational, 1,194 women):
- Higher isoflavone intake from diet associated with:
- 3% higher lumbar spine BMD
- 5% higher femoral neck BMD
Dosing and Sources
Supplement dose: 50-100mg isoflavones daily (higher doses may be more effective)
Soy food sources:
| Food | Isoflavone Content |
|---|---|
| Tofu (3 oz) | 30-40mg |
| Tempeh (3 oz) | 60mg |
| Edamame (1/2 cup) | 30mg |
| Soy milk (1 cup) | 25mg |
| Miso (2 tbsp) | 40mg |
Food vs supplements: Both effective; food provides additional nutrients (protein, fiber, minerals)
Best Soy Isoflavone Supplements
Quality options:
- NOW Foods Soy Isoflavones: 150mg per serving
- Bluebonnet Soy Isoflavones: Non-GMO
- Jarrow Formulas Iso-Rich Soy: Standardized extract
Combination bone formulas with soy:
- Some bone health formulas include soy isoflavones + calcium + D3
Cost: $10-20/month
Safety and Controversy
Safety profile:
- Generally well-tolerated
- Minimal side effects (occasional GI discomfort)
Controversial concerns:
Breast cancer risk?
- Current evidence: Soy does NOT increase breast cancer risk
- May actually be protective (observational studies in Asian populations)
- Even breast cancer survivors may safely consume soy (per American Cancer Society)
- But: Women with hormone-sensitive cancers should discuss with oncologist
Thyroid concerns?
- Soy may interfere with thyroid hormone absorption
- Solution: Take thyroid medication 3-4 hours away from soy
Contraindications:
- Some doctors advise caution in women taking tamoxifen (theoretical interaction)
- Soy allergy (obviously)
Drug interactions:
- May interact with thyroid medications (separate timing)
- Possible interaction with hormone therapies (discuss with doctor)
Comparison Table: Menopause Bone Health Supplements
Here's a comprehensive side-by-side comparison to guide your supplement selection:
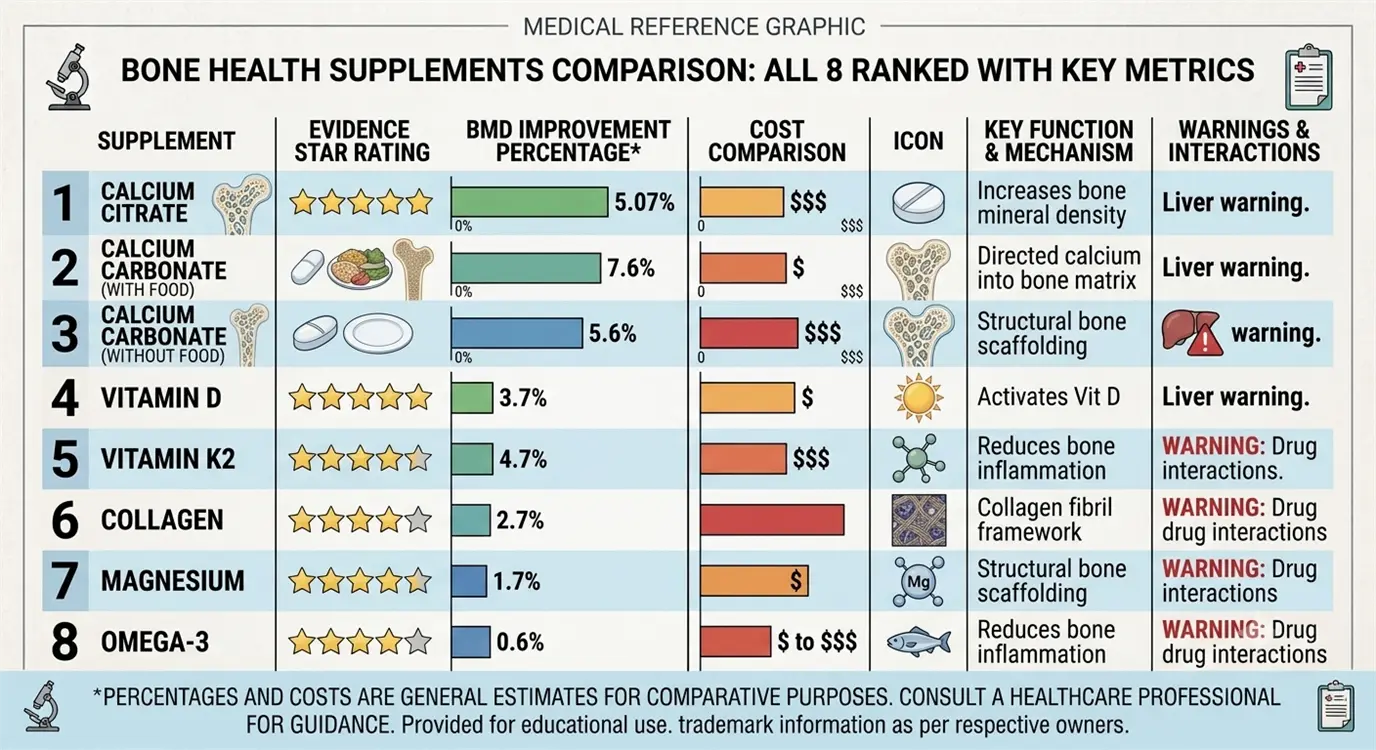
| Rank | Supplement | Key Benefit | Optimal Dosage | Evidence Level | Monthly Cost | Best For |
|---|---|---|---|---|---|---|
| #1 | Vitamin D3 + K2 | Calcium absorption + bone deposition | 2,000-5,000 IU D3 + 100-200mcg K2 | ⭐⭐⭐⭐⭐ Multiple large RCTs | $15-30 | Everyone (foundation) |
| #2 | Calcium Citrate/Carbonate | Provides bone mineral building block | 1,000-1,200mg (total with diet) | ⭐⭐⭐⭐⭐ Gold standard | $10-25 | Everyone (foundation) |
| #3 | Collagen Peptides | Bone matrix support, quality | 5-15g daily | ⭐⭐⭐⭐ Strong, emerging | $25-45 | Osteopenia, fracture risk |
| #4 | Magnesium Glycinate | Vitamin D activation, bone formation | 300-400mg | ⭐⭐⭐⭐ Well-established | $10-20 | Everyone (essential cofactor) |
| #5 | Boron | Hormone-bone synergy, mineral retention | 3-6mg daily | ⭐⭐⭐ Promising, limited large trials | $5-10 | Low estrogen, mineral loss |
| #6 | Probiotics | Gut-bone axis, inflammation | 10-20 billion CFU (L. reuteri) | ⭐⭐⭐ Emerging evidence | $20-40 | Osteopenia, gut issues |
| #7 | Omega-3 Fish Oil | Anti-inflammatory, reduces resorption | 1-2g EPA+DHA | ⭐⭐⭐ Moderate, mixed results | $20-35 | High inflammation, cardiovascular |
| #8 | Soy Isoflavones | Phytoestrogen bone protection | 50-100mg isoflavones | ⭐⭐⭐ Moderate (ethnic variation) | $10-20 | Equol producers, low-estrogen |
Potential Side Effects and Safety for Bone Supplements in Menopause
While bone health supplements are generally safe, it's important to understand potential side effects and interactions.
Common Side Effects by Supplement
Calcium:
- Constipation (10-15% of users, especially carbonate)
- Gas, bloating
- Rare: Kidney stones (pre-existing risk factors)
- Very rare: Hypercalcemia (excessive doses)
Vitamin D:
- Minimal at recommended doses
- Excess (>10,000 IU long-term): Hypercalcemia, nausea, weakness
- Rare: Kidney stones
Magnesium:
- Loose stools, diarrhea (dose-dependent, reduce if occurs)
- Usually self-limiting
Collagen:
- Minimal (excellent safety profile)
- Rare: Mild digestive upset
Others:
- Generally minimal side effects at recommended doses
Drug Interactions (Critical)
Bisphosphonates (Fosamax, Boniva, Reclast):
- Calcium, magnesium: Significantly reduce absorption
- Timing rule: Take bisphosphonate on empty stomach, wait 60 minutes before any supplements/food
Thyroid Medications (Levothyroxine):
- Calcium, magnesium, soy: Reduce thyroid medication absorption
- Timing rule: Separate by 4 hours minimum
Blood Thinners (Warfarin):
- Vitamin K2: Antagonizes warfarin (CONTRAINDICATION)
- Omega-3s, boron: May enhance anticoagulation (monitor INR)
Antibiotics:
- Calcium, magnesium: Reduce antibiotic absorption
- Timing rule: Separate by 2-4 hours
Safety Monitoring
Who should be monitored more closely:
- Women with kidney disease (calcium, vitamin D, magnesium)
- History of kidney stones (calcium, vitamin D)
- Hypercalcemia risk (calcium, vitamin D)
- On anticoagulants (vitamin K2, omega-3s)
- Hormone-sensitive cancers (soy isoflavones - discuss with oncologist)
Recommended testing:
- Baseline: Vitamin D level (25-hydroxyvitamin D), calcium, magnesium
- Follow-up: Recheck vitamin D after 3 months of supplementation
- Annual: Vitamin D, calcium, basic metabolic panel
Stacking Protocol: Best Supplement Combinations for Maximum BMD
Creating an effective supplement stack combines synergistic nutrients for enhanced bone protection.
Tier 1: Foundation Stack (Everyone)
Essential Core:
- Vitamin D3: 2,000-4,000 IU daily
- Vitamin K2 (MK-7): 100-200mcg daily
- Calcium Citrate: 500-600mg twice daily (total 1,000-1,200mg with diet)
- Magnesium Glycinate: 300-400mg daily
Why this combination:
- D3 + K2 work synergistically (absorption + deposition)
- Calcium provides mineral building block
- Magnesium activates D3 and balances calcium
- Cost: ~$40-60/month
- Expected benefit: Slow BMD loss by 40-60%, maintain existing density
Timeline: Start immediately; continue indefinitely
Tier 2: Enhanced Stack (Osteopenia or Higher Risk)
Core + Added:
- Tier 1 supplements (above)
- Plus: Collagen Peptides: 5-10g daily
- Plus: Boron: 3-6mg daily
Why add these:
- Collagen supports bone matrix quality (not just quantity)
- Boron enhances hormone-bone synergy, reduces mineral loss
- Addresses bone quality + density
- Cost: ~$70-100/month
- Expected benefit: Potential 1-2% BMD gains in spine/hip over 12 months
Timeline: 12+ months for full benefit
Tier 3: Comprehensive Stack (Osteoporosis or Advanced Age)
Enhanced + Added:
- Tier 2 supplements (above)
- Plus: Probiotics: 10-20 billion CFU (L. reuteri strain)
- Plus: Omega-3s: 1-2g EPA+DHA daily
Why add these:
- Probiotic gut-bone axis support
- Omega-3 anti-inflammatory protection
- Addresses all pathways of bone loss
- Cost: ~$110-150/month
- Expected benefit: Maximum BMD preservation, fracture risk reduction
Timeline: 12-24 months for full benefit; maintain long-term
Optional Add-Ons (Based on Individual Needs)
Add Soy Isoflavones if:
- Very low estrogen symptoms
- Asian descent (higher equol producer likelihood)
- No contraindications (breast cancer history, thyroid issues)
- Dose: 50-100mg isoflavones daily
Timing and Administration Tips
Morning routine:
- Vitamin D3 + K2 (with breakfast containing fat)
- Calcium 500-600mg (with or after breakfast)
- B vitamins (if taking for energy)
- Collagen (in coffee/smoothie)
Evening routine:
- Magnesium 300-400mg (30-60 min before bed for sleep benefit)
- Calcium 500-600mg (with dinner)
- Omega-3s (with dinner)
Anytime:
- Probiotics (empty stomach 30 min before meal, or as directed)
- Boron (with any meal)
Important Stacking Rules
Do:
- Split calcium doses (max 600mg per dose for absorption)
- Take fat-soluble vitamins (D, K, omega-3) with meals containing fat
- Maintain consistent daily schedule
- Track symptoms and adjust as needed
Don't:
- Exceed upper limits (especially calcium, vitamin D)
- Take all supplements in single massive dose
- Forget to test vitamin D levels (personalize dose)
- Neglect diet and exercise (supplements complement, don't replace)
Diet and Exercise to Enhance Bone Health Supplements
Supplements work best when combined with bone-supporting lifestyle habits.
Dietary Strategies
Calcium-rich foods (aim for 600-800mg from diet):**
- Dairy: Yogurt, milk, cheese
- Leafy greens: Kale, collards, bok choy
- Fortified foods: Orange juice, plant milks, cereals
- Fish with bones: Sardines, canned salmon
- Sesame seeds, almonds
Vitamin K-rich foods:
- Dark leafy greens (kale, spinach, Swiss chard)
- Broccoli, Brussels sprouts, cabbage
- Fermented foods (natto has highest K2)
Protein (essential for bone matrix, aim 1-1.2g per kg body weight):
- Lean meats, poultry, fish
- Eggs, dairy
- Legumes, tofu, tempeh
Avoid/Limit:
- Excessive salt (increases calcium excretion)
- Excess caffeine (>3-4 cups coffee may reduce absorption)
- Alcohol (>2 drinks daily impairs bone formation)
- High-sugar foods (inflammatory)
Exercise Protocols for Bone Density
Weight-bearing aerobic exercise:
- Walking, jogging: 30 min daily, 5x/week
- Dancing, hiking: Fun alternatives
- Stair climbing: High-impact, effective
- Impact: Mechanical stress signals bones to strengthen
Resistance training (MOST IMPORTANT):
- 2-3x weekly, all major muscle groups
- Progressive overload: Gradually increase weight
- Focus: Hip-loading exercises (squats, lunges), spine-loading (deadlifts, rows)
- Impact: Direct bone stimulation at vulnerable fracture sites
Balance training (fracture prevention):
- Tai chi, yoga
- Single-leg stands
- Reduces fall risk (50% of fractures result from falls)
Example weekly schedule:
- Monday: Resistance training (full body)
- Tuesday: Walk 30 min
- Wednesday: Yoga or tai chi
- Thursday: Resistance training
- Friday: Walk 30 min
- Saturday: Activity of choice (hiking, dancing)
- Sunday: Rest or gentle yoga
Frequently Asked Questions (FAQ)
Q1: What is the best supplement for bone health during menopause?
Answer: The single best supplement is Vitamin D3 + K2 (2,000-5,000 IU D3 + 100-200mcg K2 daily).
Why this combination wins:
- Addresses the most common deficiency (75% of postmenopausal women are vitamin D deficient)
- Strongest clinical evidence (multiple large RCTs showing BMD improvements)
- Vitamin D increases calcium absorption by 30-80%
- Vitamin K2 ensures calcium deposits in bones (not arteries)
- Synergy provides 1-2% BMD gains in lumbar spine
- Essential foundation for all other bone supplements to work
However, bone health requires a comprehensive approach:
The most effective strategy combines:
- Vitamin D3 + K2 (calcium absorption & deposition)
- Calcium (mineral building block)
- Magnesium (activates vitamin D, supports bone formation)
- Collagen peptides (bone matrix support)
Think of it like building a house:
- Vitamin D+K2 = foundation
- Calcium = bricks
- Magnesium = mortar
- Collagen = structural framework
No single supplement replaces a complete protocol, but if choosing only one, D3+K2 is non-negotiable.
Q2: How much vitamin D for menopause bone loss?
Answer: 2,000-5,000 IU daily for most postmenopausal women, personalized based on blood test results.
Detailed dosing guide:
Step 1: Get Tested
- Measure 25-hydroxyvitamin D blood level
- Test before supplementing (establishes baseline)
Step 2: Dose Based on Current Level
| Current Level | Status | Recommended Dose |
|---|---|---|
| <20 ng/mL | Deficient | 5,000-10,000 IU daily (12 weeks), then retest |
| 20-30 ng/mL | Insufficient | 4,000-5,000 IU daily |
| 30-40 ng/mL | Adequate | 2,000-4,000 IU daily (maintenance) |
| 40-60 ng/mL | Optimal for bones | 2,000-3,000 IU daily (maintain) |
| >60 ng/mL | High (no benefit) | 1,000-2,000 IU or reduce |
Target for bone health: 40-60 ng/mL (100-150 nmol/L)
Why individualization matters:
- Body weight (heavier individuals need more)
- Sun exposure (less exposure = more supplementation needed)
- Age (absorption decreases with age)
- Skin tone (darker skin requires more)
- Geographic location (northern latitudes need more)
Retest schedule:
- Recheck after 3 months of supplementation
- Once optimal, recheck annually
Important: Higher isn't always better—levels above 60 ng/mL show no additional bone benefit and may increase fall risk.
Safety note: 10,000 IU daily long-term can cause toxicity; stay under 5,000 IU for maintenance unless medically supervised.
Q3: Do calcium supplements prevent fractures in menopause?
Answer: Calcium supplements reduce fracture risk by 12-24% when combined with vitamin D, but results are modest and debated—calcium alone shows minimal benefit.
The evidence:
2015 Meta-Analysis (59 RCTs, 12,000+ women):
- Calcium alone: 12% fracture reduction (not statistically significant in all studies)
- Calcium + Vitamin D: 24% fracture reduction (significant)
- Greatest benefit in women with:
- Very low baseline calcium intake (<600mg/day from diet)
- Vitamin D deficiency
- Existing osteoporosis
2017 U.S. Preventive Services Task Force (USPSTF) Conclusion:
- Insufficient evidence to recommend calcium/vitamin D supplements for PRIMARY fracture prevention in healthy postmenopausal women
- BUT: May benefit women with osteoporosis or very low dietary intake
Why the debate?
Limitations of calcium supplementation:
- Only addresses one aspect of bone health (mineral content)
- Doesn't improve bone quality/matrix
- May increase cardiovascular event risk at high doses (controversial)
- Dietary calcium may be superior to supplements
When calcium supplements likely help:
- Dietary calcium intake <600mg/day
- Combined with vitamin D (synergy essential)
- Part of comprehensive approach (exercise, other supplements)
- Early intervention (perimenopause/early menopause)
Bottom line:
- Calcium supplements are not a magic bullet for fracture prevention
- Most effective when:
- Combined with vitamin D
- Part of multi-nutrient protocol
- Alongside weight-bearing exercise
- Started early in menopause transition
- Focus on total calcium intake (diet + supplements) rather than supplements alone
- Target 1,200mg total daily (aim for 600-800mg from food, supplement the gap)
Better fracture prevention strategies:
- Vitamin D optimization (more impactful than calcium alone)
- Resistance exercise 2-3x weekly (strongest evidence for fracture reduction)
- Fall prevention (balance training, home safety)
- Bone quality supplements (collagen, magnesium, K2)
Q4: Are probiotics good for bone health post-menopause?
Answer: Yes, emerging evidence shows specific probiotic strains—particularly Lactobacillus reuteri—can preserve bone density in postmenopausal women, though this is a newer area of research.
Clinical evidence:
2017 Swedish Study (90 women, 12 months):
- Lactobacillus reuteri (10 billion CFU) daily
- Results:
- 50% reduction in lumbar spine BMD loss vs placebo
- Placebo lost 1.0%; probiotic group lost only 0.5%
- No adverse effects
2022 Meta-Analysis (14 RCTs, 1,143 women):
- Probiotics significantly improved lumbar spine BMD
- Greater benefits in women with osteopenia
- Best results with Lactobacillus strains
How probiotics support bones:
1. Enhance mineral absorption:
- Produce short-chain fatty acids (SCFAs) that improve calcium absorption
- Lower intestinal pH (better mineral bioavailability)
- Synthesize vitamin K2 in gut
2. Reduce inflammation:
- Decrease pro-inflammatory cytokines (TNF-α, IL-6) that activate osteoclasts
- Modulate immune system to reduce bone-destroying inflammation
3. Influence hormone metabolism:
- Affect estrogen metabolism and recycling
- May improve utilization of existing estrogen
Best probiotic strains for bones:
- Lactobacillus reuteri (strongest evidence)
- Lactobacillus casei
- Bifidobacterium longum
- Multi-strain formulas may provide broader benefits
Recommended protocol:
- Dose: 10-20 billion CFU daily
- Form: Supplement + probiotic-rich foods (yogurt, kefir, sauerkraut)
- Duration: Minimum 6-12 months for bone benefits (chronic supplementation needed)
Important caveats:
- This is an emerging field—more large, long-term studies needed
- Probiotics are complementary (not a replacement for D3, calcium, exercise)
- Individual response varies (microbiome diversity matters)
- Best results when part of comprehensive bone health protocol
Who may benefit most:
- Women with osteopenia
- Those with gut issues (IBS, dysbiosis)
- Post-antibiotic treatment
- Low dietary calcium absorption
Safety: Excellent safety profile; minimal side effects (occasional gas/bloating initially)
Q5: When should I start bone supplements in perimenopause?
Answer: Ideally during perimenopause (40s) or within first 5 years of menopause—the earlier, the better for maximum protection.
Why timing matters:
Perimenopause (ages 40-50):
- Bone loss begins accelerating as estrogen fluctuates (even before final period)
- Early intervention can slow or prevent initial BMD decline
- Easier to preserve existing bone than rebuild lost density
First 5-7 years post-menopause (ages 50-57):
- Critical window—most rapid bone loss occurs (2-3% annually)
- Intervention during this period has maximum impact
- Slowing loss now prevents osteoporosis later
After 7 years post-menopause:
- Still beneficial, but harder to make significant BMD gains
- Focus shifts to fracture prevention rather than BMD improvement
- May require prescription medications (bisphosphonates) if osteoporosis present
Evidence for early intervention:
- Women who start calcium+D3 in early menopause have 40% less bone loss over 10 years vs those who start later
- Prevention is more effective than treatment
Recommended timeline:
Age 40-45 (Perimenopause):
- Start foundation supplements:
- Vitamin D3 (2,000-4,000 IU) + K2 (100mcg)
- Calcium (if dietary intake <800mg)
- Magnesium (300mg)
- Begin weight-bearing exercise routine
- Goal: Prevent bone loss before it accelerates
Age 45-52 (Late Perimenopause/Early Menopause):
- Continue foundation
- Consider adding:
- Collagen peptides (5-10g)
- Boron (3mg)
- Goal: Minimize BMD loss during critical window
Age 52+ (Postmenopause):
- Continue all supplements
- Consider comprehensive stack (+ probiotics, omega-3s)
- Get baseline DEXA scan at age 50-55
- Goal: Maintain bone density, prevent fractures
Special considerations:
Start immediately if you have:
- Family history of osteoporosis
- Early menopause (<45 years)
- Low body weight (<120 lbs / 54 kg)
- History of eating disorders or amenorrhea
- Long-term steroid use
- Smoking history
- Excessive alcohol consumption
- Sedentary lifestyle
Bottom line:
- Best time to start: Perimenopause (40s)
- Second best: Early menopause (50s)
- Third best: Right now (regardless of age)
Never too late to start, but earlier = greater benefit. Even women in their 60s-70s benefit from supplementation for fracture prevention.
Final Recommendations: Personalized Bone Health Stack for 2026
After reviewing all evidence, here's your personalized action plan based on bone health status:
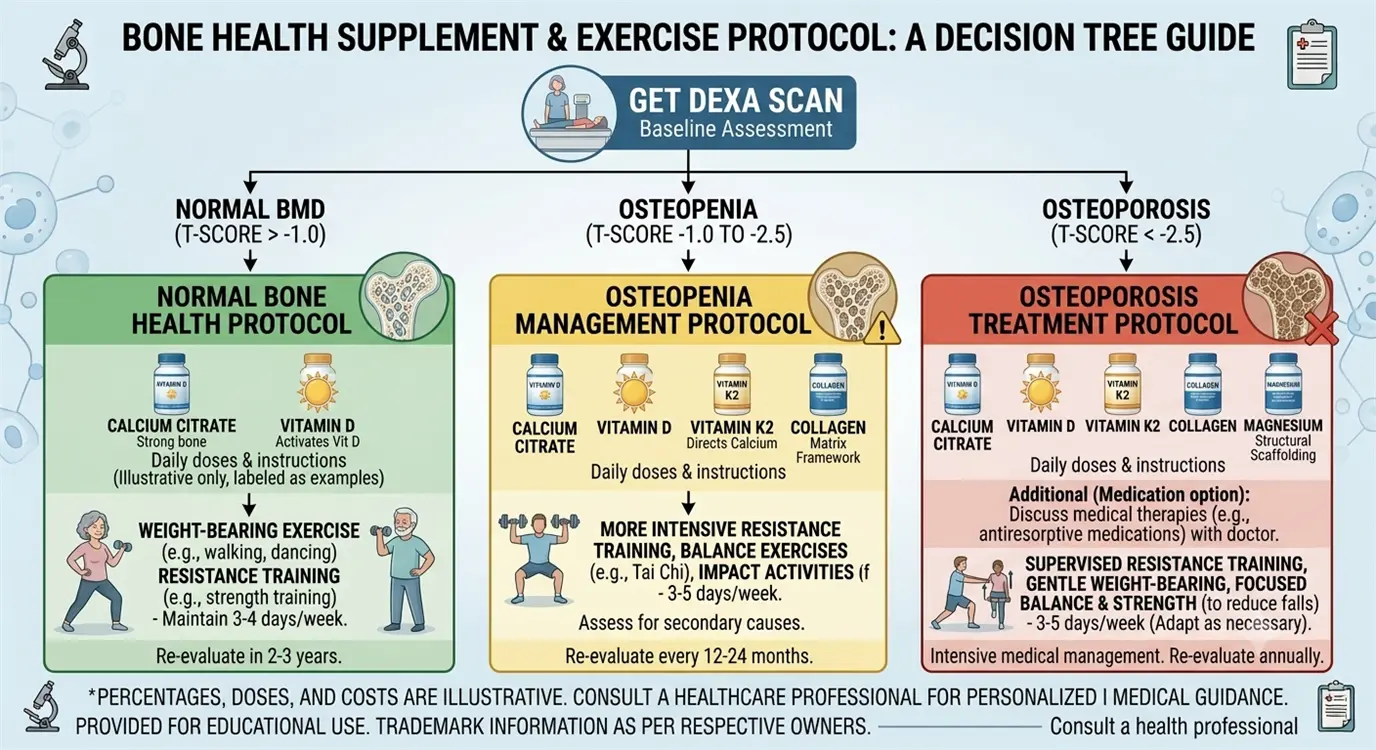
Tier 1: Prevention Protocol (Normal Bone Density)
If you have normal BMD (T-score > -1.0):
Essential Foundation:
- Vitamin D3 + K2: 2,000-4,000 IU D3 + 100mcg K2 daily
- Calcium: 500-600mg citrate twice daily (1,000-1,200mg total with diet)
- Magnesium Glycinate: 300-400mg daily
Lifestyle:
- Weight-bearing exercise 5x/week
- Resistance training 2-3x/week
- Balanced diet with adequate protein
Cost: ~$40-60/month
Goal: Maintain BMD, prevent decline
Tier 2: Osteopenia Protocol (T-score -1.0 to -2.5)
If you have low bone density (osteopenia):
Foundation + Enhancement:
- Tier 1 supplements (above)
- Plus: Collagen Peptides: 5-10g daily
- Plus: Boron: 3-6mg daily
- Plus: Probiotics: 10-20 billion CFU (L. reuteri)
Lifestyle:
- Intensive resistance training (progressive overload)
- High-impact weight-bearing (if tolerated)
- Optimize protein intake (1.0-1.2g/kg)
Monitoring:
- DEXA scan every 1-2 years
- Vitamin D level check annually
Cost: ~$90-120/month
Goal: Slow or reverse BMD loss, avoid osteoporosis
Tier 3: Osteoporosis Protocol (T-score < -2.5)
If you have osteoporosis:
Comprehensive Stack:
- All Tier 2 supplements (above)
- Plus: Omega-3s: 1-2g EPA+DHA daily
- Plus: Soy Isoflavones: 50-100mg daily (if no contraindications)
Medical Management:
- Consult doctor about prescription medications (bisphosphonates, denosumab, teriparatide)
- Supplements complement but may not replace medical treatment
- Fracture risk assessment (FRAX score)
Lifestyle:
- Modified exercise (avoid high-impact; focus on resistance + balance)
- Fall prevention strategies
- Home safety modifications
Monitoring:
- DEXA scan annually
- Blood work every 6 months
- Close medical supervision
Cost: ~$120-160/month (supplements + medical care)
Goal: Prevent fractures, stabilize or improve BMD
Critical Next Steps
1. Get Baseline Testing:
- DEXA scan (age 50-55 or earlier if risk factors)
- Vitamin D level (25-hydroxyvitamin D)
- Calcium, magnesium serum levels
- Consider: Bone turnover markers (CTX, P1NP) if osteopenia/osteoporosis
2. Personalize Your Protocol:
- Start with Tier 1 (everyone)
- Add tiers based on DEXA results
- Adjust based on lab values
3. Prioritize Lifestyle:
- Exercise is non-negotiable—supplements alone insufficient
- Weight-bearing + resistance training = 50% of fracture prevention
- Diet provides 600-800mg calcium naturally
4. Monitor Progress:
- Track symptoms subjectively (energy, overall health)
- Recheck vitamin D after 3 months
- DEXA scan in 1-2 years to assess BMD changes
5. Consult Healthcare Provider:
- Discuss supplement plan (especially if taking medications)
- Review DEXA results together
- Determine if prescription medications needed
Take Action for Your Bone Health Today
Bone loss during menopause is not inevitable—it's preventable and treatable with the right approach.
The key takeaway: Start early, be consistent, and use a comprehensive strategy combining:
- ✓ Evidence-based supplements (D3+K2, calcium, magnesium, collagen as foundation)
- ✓ Weight-bearing and resistance exercise (non-negotiable)
- ✓ Bone-supporting nutrition
- ✓ Regular monitoring (DEXA scans, lab work)
- ✓ Medical supervision when needed
Your bones are worth the investment—both in supplements and effort. The cost of prevention ($40-120/month) pales in comparison to the cost of hip fractures, vertebral compression, and loss of independence.
Don't wait until osteoporosis develops. Begin your bone health protocol today, and give your skeleton the support it needs during the menopause transition and beyond.
Disclaimers
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. The supplement recommendations have not been evaluated by the Food and Drug Administration and are not intended to diagnose, treat, cure, or prevent any disease.
Always consult with a qualified healthcare professional before starting any new supplement regimen, especially if you have pre-existing medical conditions, take medications, or have risk factors for osteoporosis. Individual results may vary, and what works for one woman may not work for another.
DEXA scans and medical supervision are essential for proper bone health management. Supplements complement—but do not replace—medical treatment when osteoporosis is present. Your healthcare provider can help create a personalized plan based on your unique health profile and bone density status.
Third-Party Product Disclaimer
Product recommendations in this article are based on quality, evidence, and third-party testing. We are not affiliated with or compensated by any brands mentioned. Always verify product quality and consult healthcare providers before purchasing supplements.