Published on Medium | Estimated read time: 12 minutes | Category: Women's Health & Wellness
Medical Disclaimer: This article is for informational purposes only. Always consult a qualified healthcare provider before starting any new supplement regimen, especially if you are managing a medical condition or taking prescription medications.

Why Hormonal Shifts Lead to Extreme Estrogen-Deficient Skin Dryness
If your skin has become noticeably drier, thinner, or persistently itchy in recent years, you are not imagining it — and you are not alone. Millions of women transitioning through perimenopause and into postmenopause experience a profound shift in the quality, thickness, and moisture levels of their skin. This is not a surface-level problem that a richer face cream can solve. It is a systemic, biology-driven change rooted in one of the most significant hormonal transitions the human body undergoes.
The decline of estrogen — particularly 17β-estradiol — fundamentally alters how skin is built, maintained, and hydrated at the cellular level. The tissues that once produced collagen efficiently, retained water in their matrix, and renewed themselves regularly are now operating in a hormonal environment that no longer supports those processes. The result is skin that feels tight, rough, fragile, and persistently uncomfortable.
Understanding why this happens is the first step toward addressing it effectively. Because the most powerful interventions for menopausal dry skin are not topical — they are systemic. They work from the inside out, delivering the biological raw materials your skin can no longer produce on its own.
Why Menopause Triggers Cutaneous Dehydration and Pruritus
Menopausal skin changes are not merely cosmetic. They reflect real structural deterioration happening across multiple layers of the skin simultaneously. Two interconnected biological failures drive the experience of dryness, thinning, and itching: the collapse of the collagen-estrogen loop and the breakdown of the epidermal lipid barrier.
The Estrogen-Collagen Loop: Fibroblast Decline and Skin Thinning
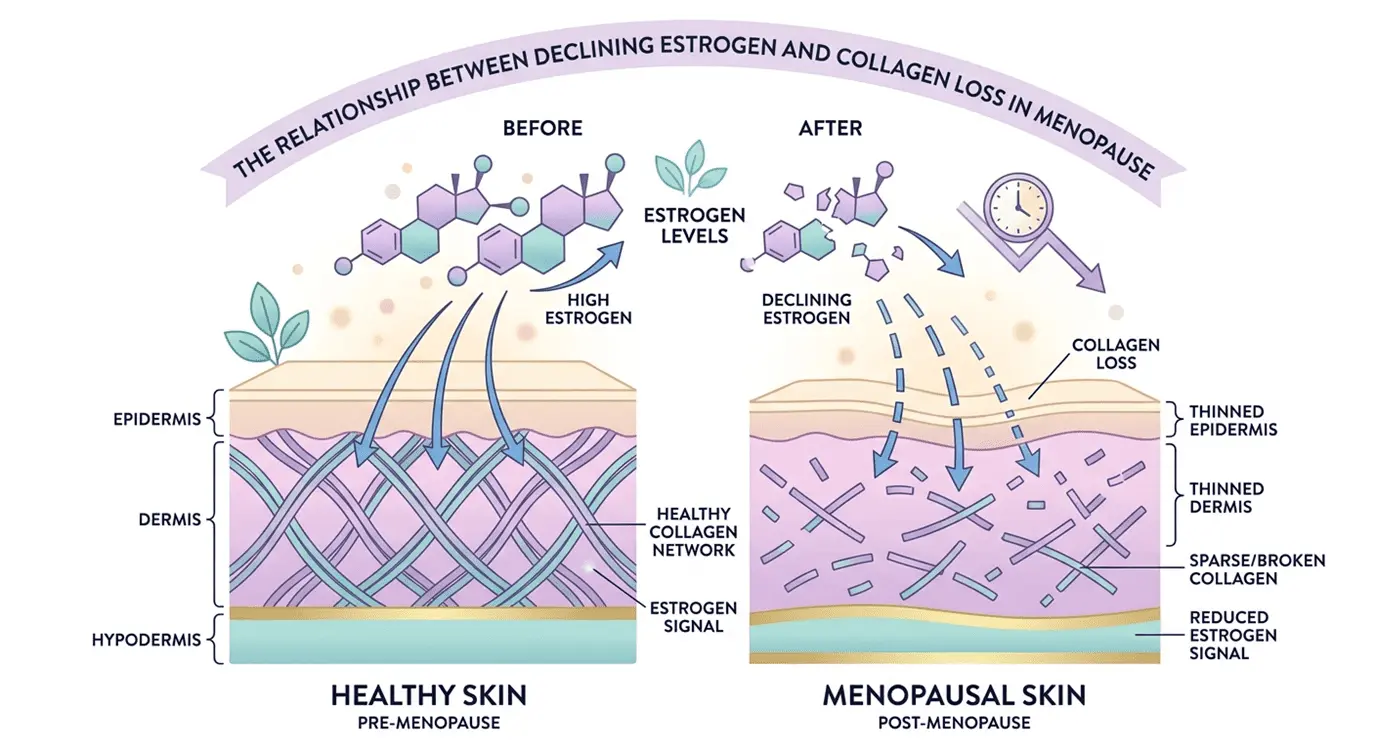
Estrogen is not simply a reproductive hormone — it is a master regulator of skin architecture. In its most biologically active form, 17β-estradiol binds to estrogen receptor beta (ER-β) found in dermal fibroblasts, the cells responsible for producing collagen, elastin, and hyaluronic acid. When estrogen binds these receptors, it activates the transcription of genes encoding structural proteins that give skin its thickness, bounce, and ability to retain moisture.
When estrogen levels fall, this signaling chain breaks down. Fibroblast activity declines, and collagen synthesis slows substantially. Research indicates that skin loses approximately 2% of its total collagen content per year during the first five years after menopause. Over a decade, this translates to a measurable reduction in skin thickness, a loss of elasticity, and the formation of fine lines that are driven not by sun exposure alone, but by internal structural depletion.
This is why topical retinoids and serums — while useful — cannot fully compensate. They act on the surface of a structure that is being hollowed from within.
The Lipid Barrier Crisis: Transepidermal Water Loss and Sebum Depletion
The second major mechanism driving menopausal skin dryness is the breakdown of the stratum corneum's lipid barrier — the outermost layer of skin, which functions as a waterproof seal for underlying tissue.
Healthy skin produces sebum, a complex mixture of oils, wax esters, and lipids secreted by sebaceous glands. This sebum, combined with ceramides, free fatty acids, and cholesterol produced within the skin itself, creates a semi-permeable barrier that limits transepidermal water loss (TEWL) — the passive evaporation of water from beneath the skin's surface. During menopause, sebaceous gland activity drops significantly as androgenic and estrogenic signaling that sustains these glands weakens. The lipid barrier becomes depleted, porous, and functionally impaired.
The consequences are direct: water escapes more rapidly from the dermis and epidermis, skin surface pH rises, and cutaneous nerve endings — no longer cushioned by a healthy lipid coat — become hypersensitized. This hypersensitivity manifests as menopausal pruritus: chronic itching that intensifies at night, in dry environments, and after bathing.
Women also experiencing mucosal dryness alongside cutaneous symptoms may be presenting features of Genitourinary Syndrome of Menopause (GSM), a related condition driven by the same hormonal depletion affecting vaginal and urinary tract tissue.
Systemic Interventions: The Best Oral Supplements for Menopausal Dry Skin
Rebuilding the skin's structure, locking in moisture, and calming systemic inflammation requires interventions that reach the dermis — not just the epidermis. The following supplement classes have the strongest clinical evidence base for addressing the root biological causes of menopausal skin dryness.
| Supplement Class | Daily Dosage | Primary Mechanism | Expected Outcome |
|---|---|---|---|
| Hydrolyzed Collagen Peptides (Types I & III) | 2.5g – 10g | Stimulates fibroblast collagen synthesis | Increased dermal thickness, elasticity |
| Oral Hyaluronic Acid | 120mg – 240mg | Retains water in the extracellular matrix | Improved surface and deep hydration |
| Omega-3 Fatty Acids (EPA & DHA) | 250mg – 1,000mg | Reduces inflammatory markers; stabilizes cell membranes | Lipid barrier restoration, reduced pruritus |
| GLA (Borage / Evening Primrose Oil) | 500mg – 1,000mg | Converts to anti-inflammatory DGLA | Smoother skin, reduced sensitivity |
| Sea Buckthorn Oil (Omega-7) | 300mg – 2,000mg | Supports mucosal and cutaneous membrane integrity | External skin and urogenital hydration |
| Soy Isoflavones (Phytoestrogens) | 40mg – 80mg | Weak ER-β agonist activity | Reduced skin thinning, structural support |
| Vitamin D3 | 1,000IU – 2,000IU | Regulates epidermal cell turnover via VDRs | Barrier repair, immune-mediated dryness management |
Hydrolyzed Collagen Peptides (Types I & III) for Structural Support
Of all available supplements for menopausal skin, hydrolyzed collagen peptides have the most direct and well-documented mechanism of action. When collagen protein from marine or bovine sources is enzymatically hydrolyzed, it is broken into short-chain peptide fragments — di- and tripeptides — small enough to survive gastric digestion and cross the intestinal wall into systemic circulation.
Once in the bloodstream, these bioactive peptides accumulate preferentially in skin tissue, where they directly stimulate dermal fibroblasts. The fibroblasts interpret these peptides as signals of collagen breakdown, responding by upregulating the synthesis of new collagen, elastin, and hyaluronic acid. This mechanism has been confirmed in multiple double-blind, placebo-controlled trials.
Clinical data show that consistent supplementation with 2.5 to 10 grams of hydrolyzed collagen daily over 4 to 12 weeks produces measurable improvements in skin hydration, dermal density, and elasticity — outcomes that are particularly meaningful for postmenopausal women whose fibroblast activity is already suppressed.
Type I collagen is the dominant structural protein of the dermis. Type III collagen provides flexibility. Formulations combining both are preferable for comprehensive dermal rebuilding.
🔗 Further reading: Wrinkle reduction in post-menopausal women consuming a novel oral supplement — PubMed/NIH

Oral Hyaluronic Acid and Ceramides for Intercellular Moisture Binding
Hyaluronic acid (HA) is one of the most hydrophilic molecules in the human body, capable of retaining up to 1,000 times its own weight in water. It is a primary component of the extracellular matrix (ECM) — the gel-like scaffolding between skin cells — where it maintains the internal hydration that gives skin its plump, dewy appearance.
Topical hyaluronic acid serums are popular, but their action is restricted to the surface of the stratum corneum. Oral supplementation at 120 to 240 mg daily works differently: it increases endogenous HA synthesis and distributes hyaluronic acid throughout the extracellular matrix of the dermis, providing sustained, deep-tissue hydration that topical products cannot replicate.
Oral phytoceramides — plant-derived lipids that mirror the ceramides naturally present in the stratum corneum — offer a complementary mechanism. Research suggests these ceramides are absorbed through the intestine and migrate to the outer skin layers, where they fill in microscopic gaps in the lipid barrier, reducing TEWL and strengthening structural cohesion between skin cells.
Together, oral HA and phytoceramides address both the interior hydration deficit and the surface barrier failure characteristic of menopausal skin.
Essential Fatty Acids to Nourish the Epidermal Lipid Coat
The skin's lipid coat is not replenished by drinking more water — it is rebuilt through dietary fat intake. The three classes of essential fatty acids most relevant to menopausal skin dryness work through distinct but complementary pathways.
Omega-3 Fatty Acids (EPA and DHA) for Cellular Membrane Support and Inflammation Reduction
Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), found in high-quality fish oil and algae-based supplements, address two simultaneous problems in menopausal skin: chronic systemic inflammation and compromised cellular membrane structure.
EPA inhibits the production of pro-inflammatory signaling molecules — specifically prostaglandin E2 (PGE2) and leukotriene B4 (LTB4) — which contribute to the inflammatory pruritus many postmenopausal women experience. It also suppresses collagenase, an enzyme that degrades existing collagen. DHA integrates directly into phospholipid bilayers in skin cells, improving membrane fluidity and the cell's ability to retain moisture.
A daily dose of 250 to 1,000 mg combined EPA/DHA taken consistently over six to eight weeks typically yields noticeable improvements in skin comfort, reduced itching, and improved hydration. For those with seafood allergies, high-quality algae-derived omega-3 supplements or cold-pressed hemp seed oil are effective plant-based alternatives.
Evening Primrose and Starflower (Borage) Oils for Gamma-Linolenic Acid (GLA) Support
Gamma-linolenic acid (GLA) is a unique omega-6 fatty acid with anti-inflammatory properties that set it apart from its pro-inflammatory omega-6 counterparts. Found in high concentrations in starflower (borage) oil and evening primrose oil, GLA is metabolized in the body into dihomo-gamma-linolenic acid (DGLA), a potent anti-inflammatory compound that reinforces the structural lipids of the stratum corneum.
Clinical evidence supports taking 500 mg of evening primrose oil twice daily to relieve chronic skin roughness, heightened sensitivity, and eczema flare-ups that frequently accompany menopause. Borage oil generally contains higher GLA concentrations (~22%) than evening primrose oil (~9%), making it a more potent per-capsule option.
Sea Buckthorn Oil (Omega-7) for Mucosal and Cutaneous Hydration
Sea buckthorn oil is uniquely rich in palmitoleic acid (omega-7), a monounsaturated fatty acid that closely mimics the lipid composition of human sebum. At doses of 300 to 2,000 mg daily, sea buckthorn oil supports tissue hydration across both external skin and internal mucosal membranes — making it particularly valuable for postmenopausal women experiencing concurrent skin dryness and the mucosal atrophy associated with Genitourinary Syndrome of Menopause (GSM).

Coenzyme Q10 and Pine Bark Extract (Pycnogenol) for Advanced Cellular Defense
Two advanced antioxidant supplements deserve particular attention for their targeted benefits in postmenopausal skin.
Coenzyme Q10 (CoQ10) is a fat-soluble antioxidant produced naturally by the body, but its endogenous levels decline with age. Oral CoQ10 supplementation replenishes mitochondrial energy production in skin cells and neutralizes the free radicals responsible for accelerated cutaneous aging. Clinical trials show measurable reductions in wrinkle depth and improvements in skin smoothness after 12 weeks of consistent supplementation.
Pine Bark Extract (Pycnogenol) is one of the few botanical compounds with clinical evidence for directly upregulating skin-specific genes. Studies in postmenopausal women demonstrate that Pycnogenol stimulates the activity of hyaluronic acid synthase and type I collagen genes in the skin, producing meaningful increases in internal hydration and dermal elasticity. It also provides significant photoprotective antioxidant activity, reducing UV-induced oxidative damage in collagen-depleted mature skin.
🔗 Further reading: Complementary and Alternative Medicine for Menopause — PubMed/NIH
Micronutrient Co-Factors: Vitamins C, E, D3, Zinc, and Magnesium
High-profile supplements like collagen and omega-3s cannot function optimally without the micronutrients that support cellular repair, antioxidant protection, and barrier maintenance. During menopause, many of these cofactors become depleted simultaneously.
- Vitamin C is the single most important cofactor for collagen synthesis. Without adequate Vitamin C, the enzymatic conversion of procollagen to mature collagen cannot proceed correctly. It also acts as a water-soluble antioxidant, protecting skin cells from oxidative stress.
- Vitamin E is a fat-soluble antioxidant that resides within the lipid bilayer of skin cell membranes, protecting epidermal fats from oxidation and supporting barrier integrity.
- Vitamin D3 (1,000–2,000 IU daily) binds to nuclear Vitamin D receptors (VDRs) in skin cells, regulating the rate of epidermal cell turnover and orchestrating barrier repair processes. Low Vitamin D levels have been associated with compromised barrier function and increased inflammatory skin conditions.
- Zinc (8–15 mg daily) supports keratin synthesis, modulates cutaneous inflammation, and plays a central role in wound healing and tissue repair — all processes that slow during the postmenopausal years.
- Magnesium strengthens the skin barrier and exerts anti-inflammatory effects that help dampen the stress-induced inflammatory responses that frequently exacerbate menopausal itching.
B-Vitamin Complex for Hormonal Synthesis, Energy, and Mood Balance
The B-vitamin family provides essential metabolic support throughout the menopausal transition, with several members exerting direct and indirect effects on skin health:
- Vitamin B6 (as pyridoxal 5'-phosphate) helps regulate the estrogen-to-progesterone ratio and supports the production of neurotransmitters that manage mood fluctuations.
- Vitamin B9 (folate) has been associated with reductions in the frequency and severity of hot flashes.
- Vitamin B12 is critical for cognitive function and peripheral nerve health — absorption of B12 declines with age, making supplementation increasingly important after 50.
- Biotin (B7) supports fatty acid metabolism, ensuring that dietary and supplemental essential fatty acids are effectively metabolized and delivered to skin tissue and mucous membranes.
Endocrine-Modulating Botanicals and Phytoestrogenic Herbs
For women seeking alternatives to hormone replacement therapy (HRT) or complementary options alongside it, plant-derived phytoestrogens and botanical extracts offer meaningful, clinically investigated support.
Soy Isoflavones, Red Clover, and the Gut-Skin Axis of S-Equol
Soy- and red clover-derived isoflavones — including genistin, daidzin, and formononetin — are the most studied class of phytoestrogens. These compounds bind to estrogen receptor beta (ER-β) in skin tissue, where they partially mimic the collagen- and hyaluronic acid-stimulating effects of 17β-estradiol. At a recommended dose of 40 to 80 mg daily, soy isoflavones have been shown to reduce skin thinning and support baseline dermal density in postmenopausal women.
A critical clinical nuance: the skin benefits of dietary daidzein depend heavily on its conversion to S-equol by intestinal bacteria. S-equol has significantly higher estrogenic potency than its parent compound, and it is the primary driver of isoflavone efficacy on skin. However, fewer than 20% of Western women possess the gut microbiome composition necessary to perform this conversion. Combining phytoestrogen supplementation with probiotic strains — particularly Lactobacillus species — is therefore recommended to optimize gut-skin axis conversion and maximize clinical outcomes.
🔗 Further reading: Isoflavone Supplements for Menopausal Women: A Systematic Review — PubMed/NIH
Black Cohosh, Wild Yam, and Vitex (Chasteberry) for Systemic Endocrine Recalibration
Three additional botanicals appear commonly in menopause formulations:
Black Cohosh acts through estrogen-independent pathways — primarily via serotonergic mechanisms — to alleviate vasomotor symptoms such as hot flashes. Its direct effects on skin hydration are less well-established, and it must be avoided by individuals with liver disease.
Wild Yam (Dioscorea) supplies diosgenin, a steroid precursor historically associated with hormonal support. While often marketed as a "natural progesterone," the human body cannot convert diosgenin to progesterone directly, and clinical evidence for skin hydration benefits remains limited.
Vitex (Chasteberry) supports progesterone production via dopaminergic activity on the pituitary gland, which can help balance the estrogen-to-progesterone ratio during perimenopausal fluctuations. Its benefits are most relevant in the perimenopause phase when progesterone levels begin declining faster than estrogen.

Safety Profiling: Dosage, Quality Control, and HRT Interoperability
Because this is a YMYL (Your Money or Your Life) topic, safety must be addressed explicitly and without minimization.
Sourcing Third-Party Verified Formulations and Avoiding Synthetic Contaminants
The dietary supplement industry in most markets operates with significantly less regulatory oversight than pharmaceuticals. This means that the quality, purity, and actual dosage of supplements can vary widely between products — even products making identical claims on their packaging.
When selecting supplements for menopausal skin, prioritize products that have been tested by independent, accredited third-party organizations. Recognized certification bodies include:
- USP (United States Pharmacopeia)
- NSF International
- ConsumerLab
Third-party certification verifies that the product contains what the label states, at the dosage stated, and is free from heavy metals, synthetic fillers, undeclared ingredients, and botanical contaminants. This is not a marketing claim — it is independently audited compliance.
Drug Interactions, Hemorrhagic Risks, and HRT Interoperability
Specific safety boundaries apply to several of the supplement classes discussed:
- High-dose fish oil and Vitamin E can exert mild anticoagulant effects. Women taking prescription blood thinners (warfarin, heparin, newer anticoagulants) should consult their physician before initiating omega-3 supplementation at therapeutic doses.
- Black Cohosh carries a rare but documented risk of hepatotoxicity (liver damage). It is contraindicated in women with any history of liver disease.
- Phytoestrogens (soy isoflavones, red clover, black cohosh) must be used with caution or avoided entirely by women with a history of hormone-sensitive cancers (including estrogen receptor-positive breast cancer) or hormone-sensitive conditions. Consultation with an oncologist is mandatory before use.
- Non-hormonal supplements — including hydrolyzed collagen, oral hyaluronic acid, Vitamins C, D3, and B-complex — are highly compatible with HRT. They do not interfere with prescribed hormone dosages and offer complementary structural support that HRT alone does not provide.
Regardless of HRT status, consult a qualified general practitioner or OB-GYN before initiating a structured supplement regimen.
Complementary Top-Down Barrier Support and Holistic Habits
Systemic supplementation addresses skin dryness from the inside out, but it works best when paired with a topical skincare strategy that prevents moisture loss from the outside in.
Unscented Formulations, Barrier Ceramides, and Broad-Spectrum Sun Protection
The wrong skincare products can actively accelerate menopausal skin dryness. Products containing alcohol, synthetic fragrances, sulfates, or harsh chemical exfoliants strip the residual natural lipids from the stratum corneum, worsening TEWL and sensitizing the skin.
Switch to fragrance-free, pH-balanced cleansers and apply a barrier-rich moisturizer immediately after bathing — while the skin is still slightly damp — to trap surface moisture. Formulations containing argan oil, jojoba oil, shea butter, topical ceramides, and hyaluronic acid are most effective for postmenopausal skin.
Daily application of broad-spectrum SPF 30+ sunscreen is non-negotiable. UV exposure degrades existing collagen and elastin at a structural level, and postmenopausal skin — already collagen-depleted — is particularly vulnerable to UV-induced photoaging.
Systemic Lifestyle Habits: Dietary Proteins, Lukewarm Showers, and Air Humidifiers
Simple environmental and behavioral modifications can significantly amplify the effects of a supplement regimen:
- Hydration: Aim for 2.0 to 2.5 liters of water daily. Dehydration is directly reflected in skin turgor and surface texture.
- Shower temperature: Take short, lukewarm showers rather than prolonged hot baths. Hot water strips residual skin lipids more aggressively than cooler water.
- Humidification: A cool-mist humidifier running in sleeping or working environments mitigates the additional TEWL that dry indoor air — particularly heated winter air — accelerates.
- Dietary collagen cofactors: Consume sulfur-rich foods (broccoli, garlic, onion, eggs) alongside Vitamin C-rich foods to support endogenous collagen synthesis at the dietary level.
- Relief bathing: For acute itching flare-ups, colloidal oatmeal baths or diluted lactic acid soaks provide immediate anti-inflammatory and soothing relief without disrupting the microbiome.
FAQ: Menopause Dry Skin Supplements Explained
How long does it take for supplements to improve menopause dry skin?
Minor improvements in skin comfort can occur within two to four weeks, but the most meaningful clinical benefits — increased dermal density, improved hydration, and reduced pruritus — typically require four to eight weeks of consistent daily supplementation. Collagen peptides and phytoestrogens may require up to twelve weeks of continuous use to reach their full effect, as structural dermal rebuilding is a slow biological process.
Can I take menopause dry skin supplements alongside HRT?
Non-hormonal supplements — including hydrolyzed collagen, oral hyaluronic acid, omega-3 fatty acids, and the micronutrient cofactors (Vitamins C, D3, B-complex, zinc) — are highly compatible with HRT and provide complementary skin barrier support that hormone therapy alone does not deliver. Phytoestrogenic herbs such as soy isoflavones and red clover require prior discussion with your prescribing physician, as they can potentially interact with or amplify prescribed hormone dosages.
Are there any supplements postmenopausal women should avoid?
Women with a personal history of hormone-sensitive cancers, particularly estrogen receptor-positive breast cancer, should avoid phytoestrogens (soy isoflavones, red clover, black cohosh) unless explicitly approved by their oncologist. Women on anticoagulant therapy should exercise caution with high-dose fish oil and Vitamin E and seek medical clearance before supplementing. Black Cohosh is contraindicated in women with liver disease.
What is the single best supplement to start with for menopause itchy skin?
High-quality omega-3 fish oil is the most effective single starting point for pruritus specifically. Its anti-inflammatory action directly reduces the systemic inflammatory signaling that sensitizes cutaneous nerve endings, while its membrane-stabilizing properties restore the epidermal lipid coat that prevents moisture-triggered nerve hypersensitivity. Visible improvement in itch comfort is typically reported within six to eight weeks of consistent daily supplementation.
Does oral hyaluronic acid work as effectively as topical serums?
Oral and topical hyaluronic acid are complementary, not interchangeable. Topical low-molecular-weight HA serums provide immediate, surface-level hydration to the outer stratum corneum — an effect that is visible quickly but temporary. Oral HA supplements at 120 to 240 mg daily are clinically demonstrated to increase hyaluronic acid concentrations in the deep dermis, improving long-term, structural moisture retention in a way that no topical product can replicate. Used together, they address both the surface and the interior of the tissue simultaneously.

Synthesis: Reclaiming Cutaneous Integrity and Dermal Vitality
Menopausal dry skin is not a cosmetic inconvenience. It is a physiological consequence of systemic hormonal change — one that affects the structural proteins, lipid composition, and moisture-retention capacity of the skin at the cellular level. Topical products alone cannot reverse this decline because the source of the problem lies within the tissues they cannot reach.
A strategic, evidence-based supplement protocol — anchored by hydrolyzed collagen peptides, oral hyaluronic acid, omega-3 fatty acids, and essential micronutrient cofactors, and augmented by phytoestrogens where appropriate — provides the biological raw materials to rebuild what menopause has depleted. Paired with a barrier-protective topical regimen and consistent anti-inflammatory lifestyle habits, this inside-out approach can meaningfully restore skin comfort, thickness, and radiance.
The clinical evidence is clear: consistent, targeted supplementation over 8 to 12 weeks produces measurable improvements in all major markers of menopausal skin health — hydration, elasticity, barrier function, and pruritus reduction.
The most important next step is individualized. Consult your gynecologist, dermatologist, or integrative medicine provider to design a supplement plan calibrated to your specific health history, current medications, and symptom profile. The biological changes are real — and so is the potential to address them effectively.
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before beginning any new supplement protocol, particularly if you are managing an existing health condition or taking prescription medications.
Tags: Menopause | Women's Health | Skin Care | Supplements | Hormonal Health | Wellness | Anti-Aging | Dermatology
External Resources:
- Isoflavone Supplements for Menopausal Women: A Systematic Review — PubMed/NIH
- Complementary and Alternative Medicine for Menopause — PubMed/NIH
- A Nutraceutical Approach to Menopausal Complaints — PubMed/NIH
- Eating for Healthy Skin During Menopause — Healthline
- 8 Best Vitamins and Supplements for Dry Skin — Healthline